

Adaptive immunity and neutralizing antibodies against SARS-CoV-2 variants of concern following vaccination in patients with cancer: The CAPTURE study
- PMID: 34950880
- PMCID: PMC7612125
- DOI: 10.1038/s43018-021-00274-w
Adaptive immunity and neutralizing antibodies against SARS-CoV-2 variants of concern following vaccination in patients with cancer: The CAPTURE study
Abstract
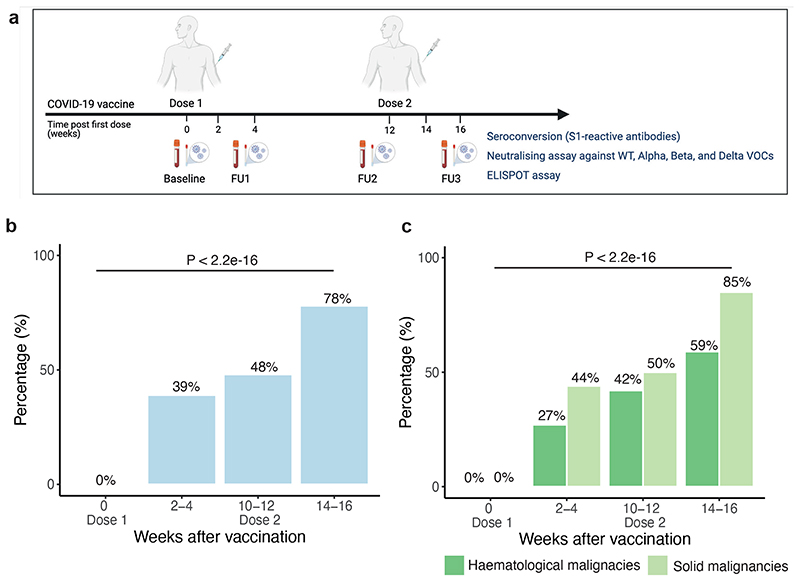
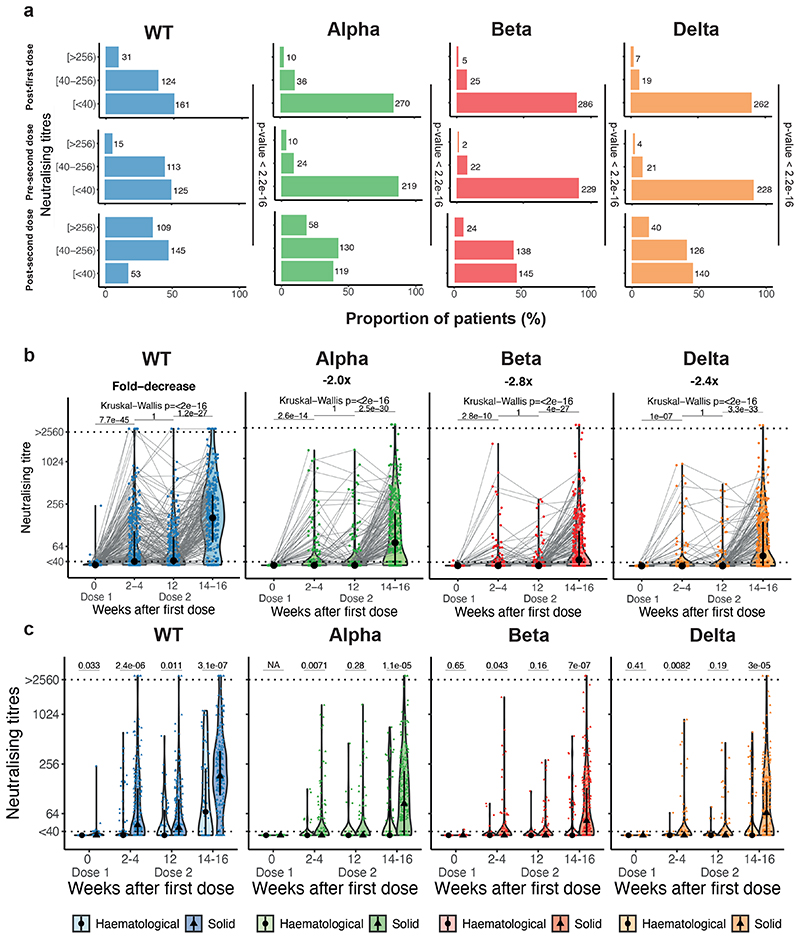
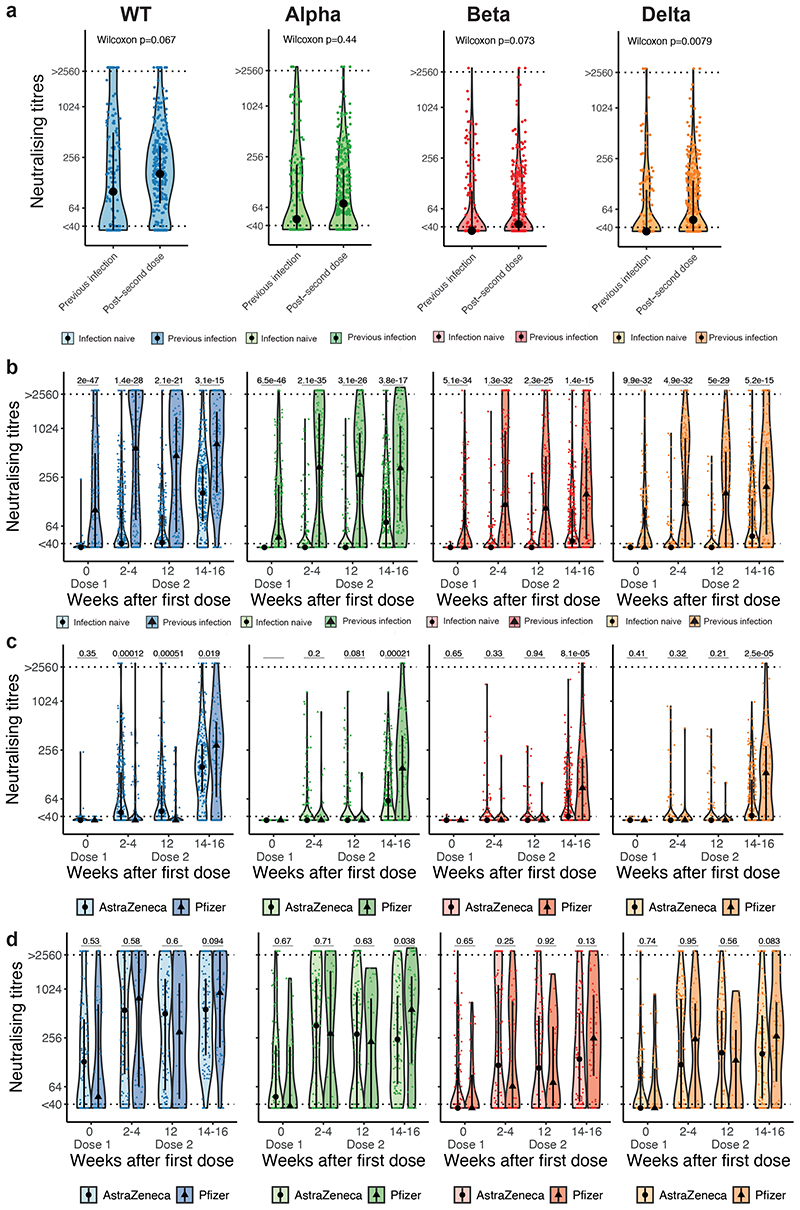
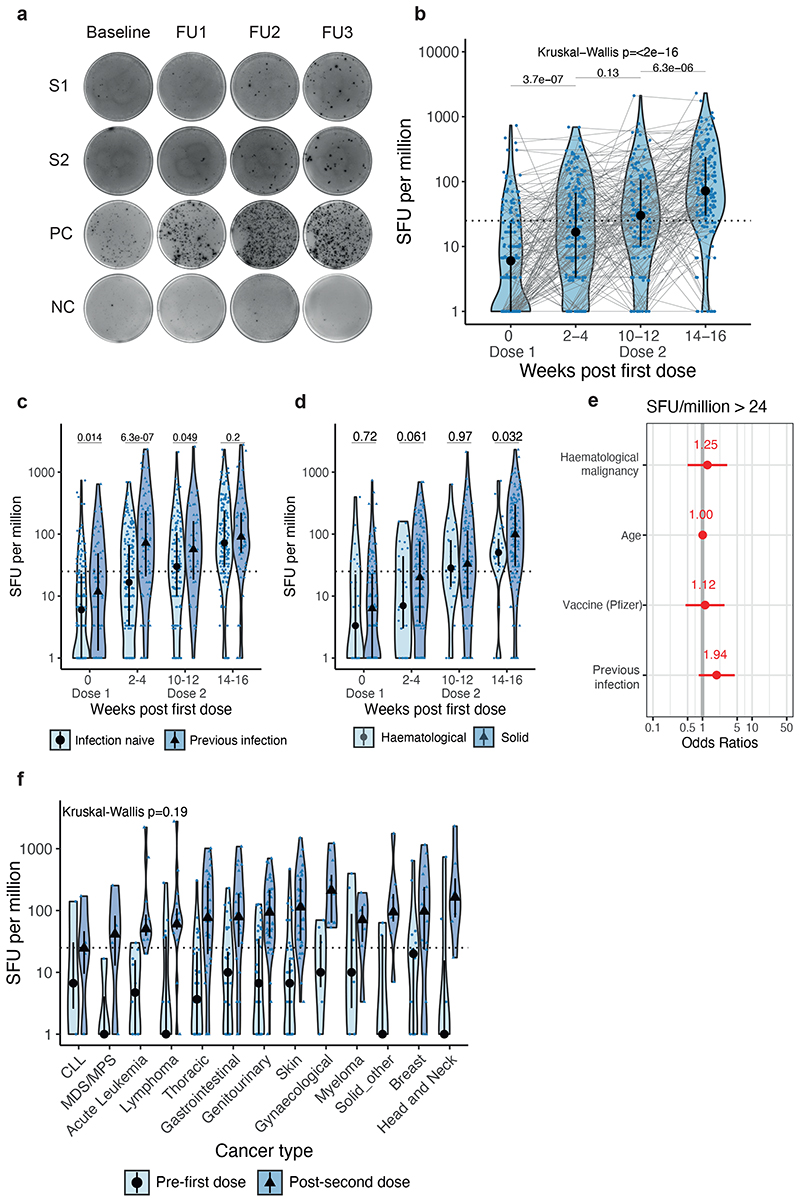
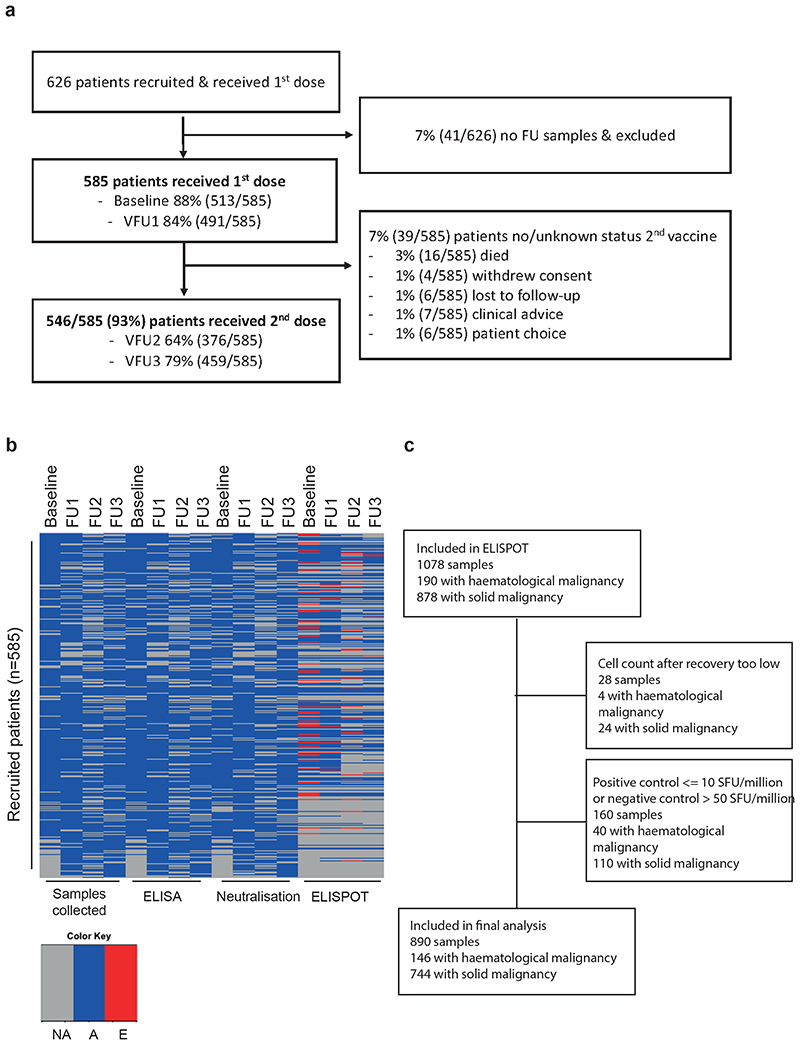
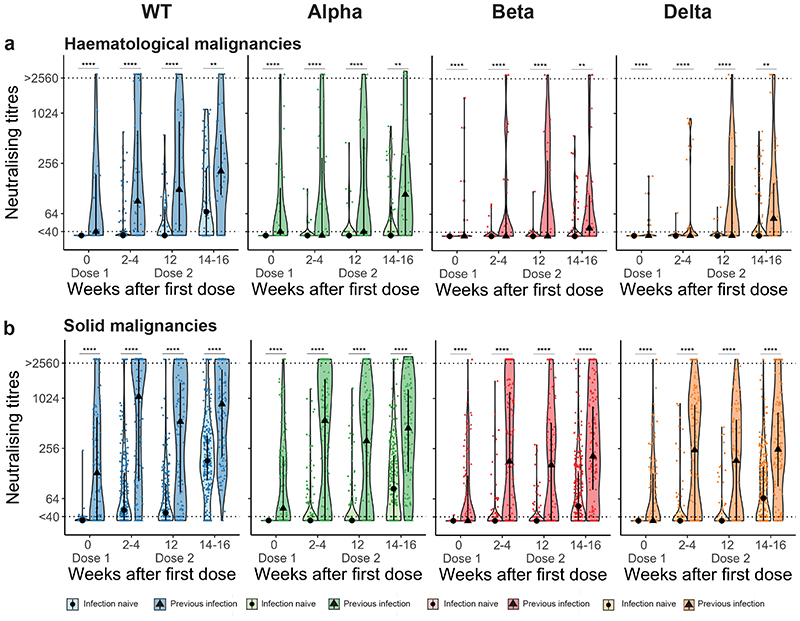
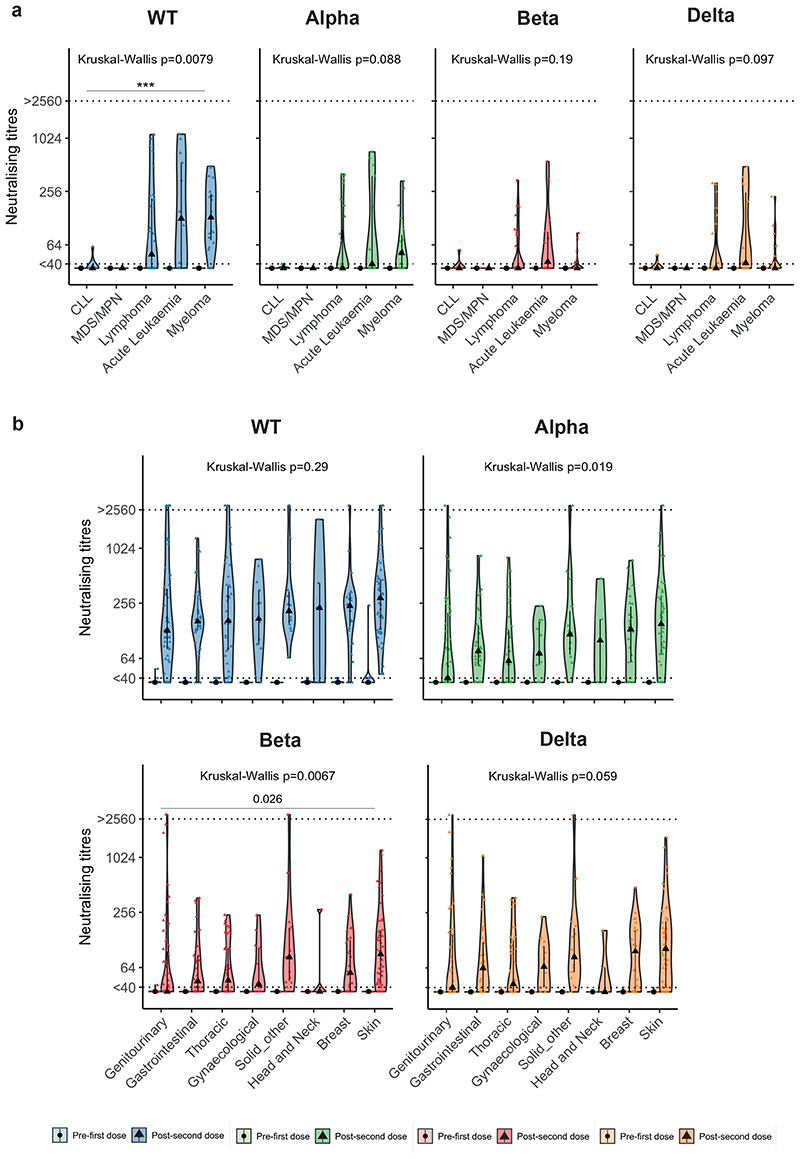
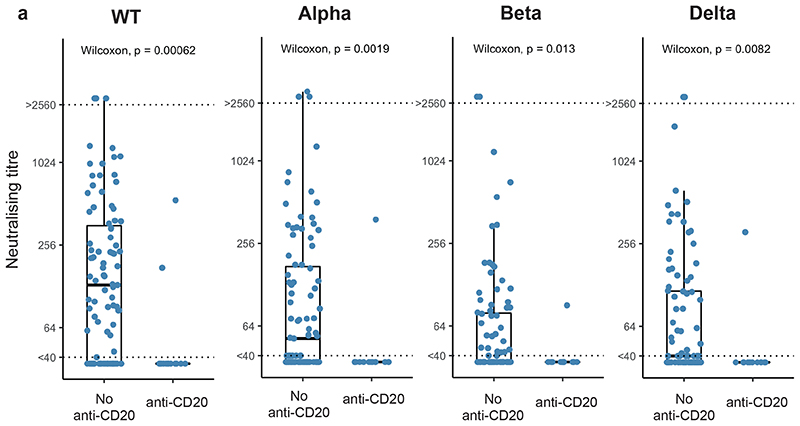
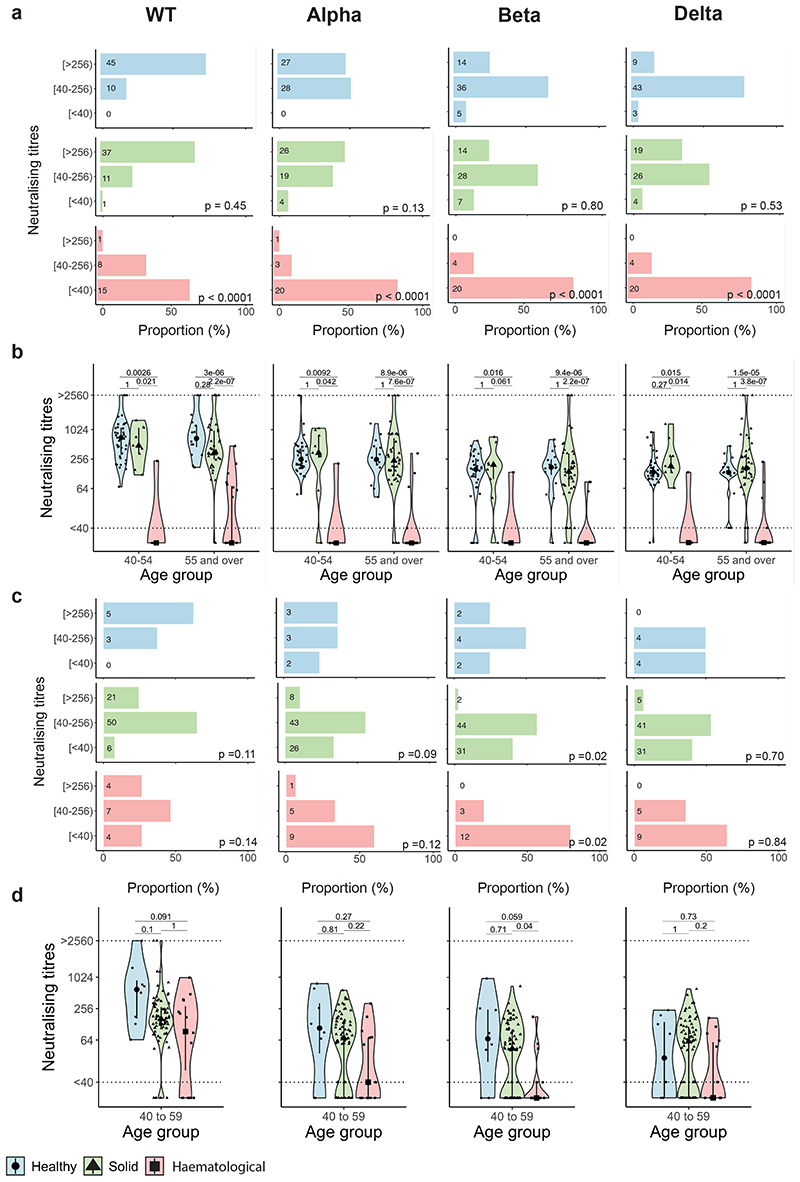
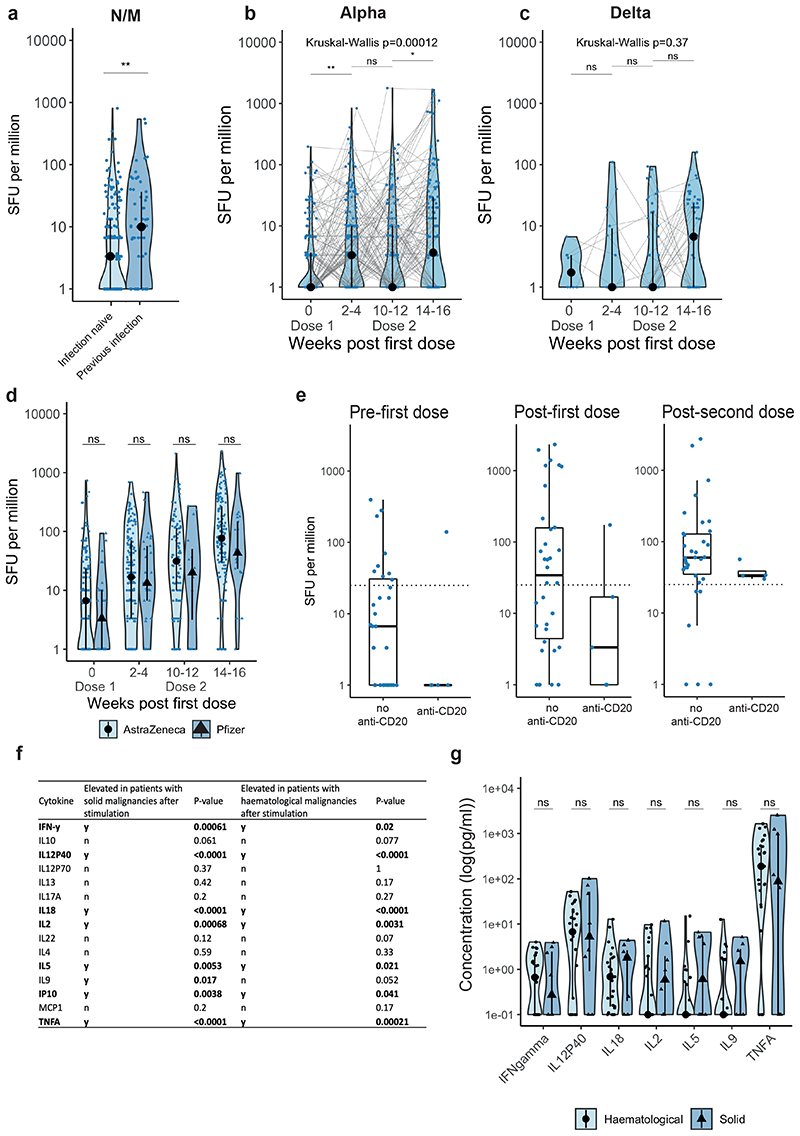
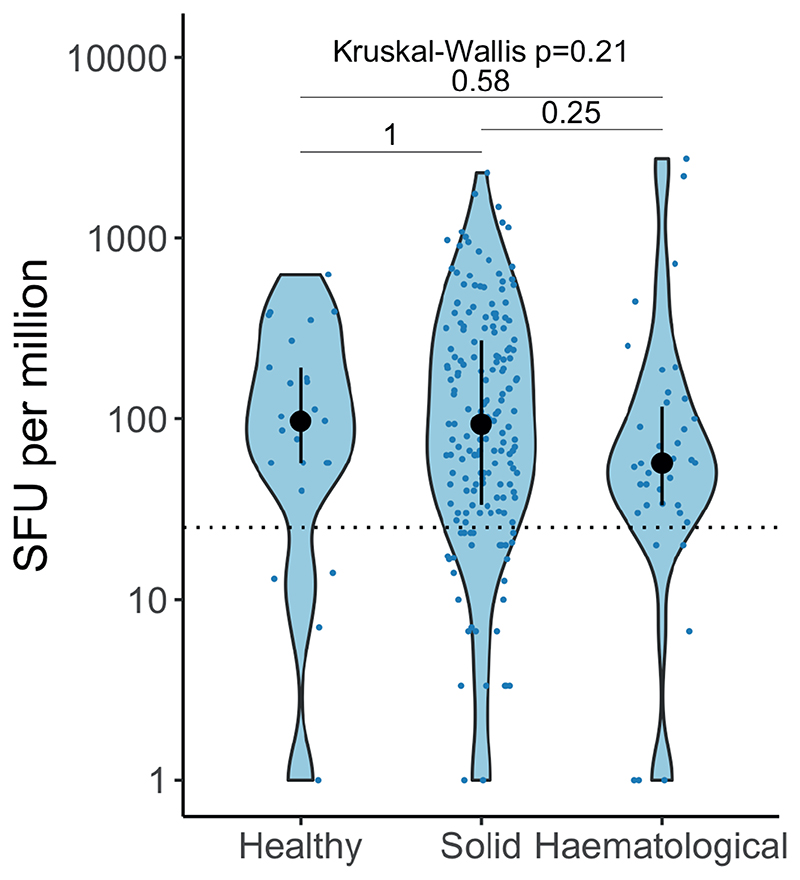
CAPTURE (NCT03226886) is a prospective cohort study of COVID-19 immunity in patients with cancer. Here we evaluated 585 patients following administration of two doses of BNT162b2 or AZD1222 vaccines, administered 12 weeks apart. Seroconversion rates after two doses were 85% and 59% in patients with solid and hematological malignancies, respectively. A lower proportion of patients had detectable neutralizing antibody titers (NAbT) against SARS-CoV-2 variants of concern (VOCs) vs wildtype (WT). Patients with hematological malignancies were more likely to have undetectable NAbT and had lower median NAbT vs solid cancers against both WT and VOCs. In comparison with individuals without cancer, patients with haematological, but not solid, malignancies had reduced NAb responses. Seroconversion showed poor concordance with NAbT against VOCs. Prior SARS-CoV-2 infection boosted NAb response including against VOCs, and anti-CD20 treatment was associated with undetectable NAbT. Vaccine-induced T-cell responses were detected in 80% of patients, and were comparable between vaccines or cancer types. Our results have implications for the management of cancer patients during the ongoing COVID-19 pandemic.
Keywords: Adaptive Immunity; Antibody Response; COVID-19; Cancer; Neutralising Antibodies; Prospective Study; SARS-CoV-2; T-cell Response; Vaccine.
Conflict of interest statement
Competing interests ST has received speaking fees from Roche, Astra Zeneca, Novartis and Ipsen. ST has the following patents filed: Indel mutations as a therapeutic target and predictive biomarker PCTGB2018/051892 and PCTGB2018/051893 and Clear Cell Renal Cell Carcinoma Biomarkers P113326GB. N.Y. has received conference support from Celegene. A.R. received a speaker fee from Merck Sharp & Dohme. J.L. has received research funding from Bristol-Myers Squibb, Merck, Novartis, Pfizer, Achilles Therapeutics, Roche, Nektar Therapeutics, Covance, Immunocore, Pharmacyclics, and Aveo, and served as a consultant to Achilles, AstraZeneca, Boston Biomedical, Bristol-Myers Squibb, Eisai, EUSA Pharma, GlaxoSmithKline, Ipsen, Imugene, Incyte, iOnctura, Kymab, Merck Serono, Nektar, Novartis, Pierre Fabre, Pfizer, Roche Genentech, Secarna, and Vitaccess. I.C. has served as a consultant to Eli-Lilly, Bristol Meyers Squibb, MSD, Bayer, Roche, Merck-Serono, Five Prime Therapeutics, Astra-Zeneca, OncXerna, Pierre Fabre, Boehringer Ingelheim, Incyte, Astella, GSK, Sotio, Eisai and has received research funding from Eli-Lilly & Janssen-Cilag. He has received honorarium from Eli-Lilly, Eisai, Servier. A.O. acknowledges receipt of research funding from Pfizer and Roche; speakers fees from Pfizer, Seagen, Lilly and AstraZeneca; is an advisory board member of Roche, Seagen, and AstraZeneca; has received conference support from Leo Pharmaceuticals, AstraZeneca/Diachi-Sankyo and Lilly. C.S. acknowledges grant support from Pfizer, AstraZeneca, Bristol Myers Squibb, Roche-Ventana, Boehringer-Ingelheim, Archer Dx Inc (collaboration in minimal residual disease sequencing technologies) and Ono Pharmaceutical, is an AstraZeneca Advisory Board member and Chief Investigator for the MeRmaiD1 clinical trial, has consulted for Amgen, Pfizer, Novartis, GlaxoSmithKline, MSD, Bristol Myers Squibb, Celgene, AstraZeneca, Illumina, Genentech, Roche-Ventana, GRAIL, Medicxi, Metabomed, Bicycle Therapeutics, and the Sarah Cannon Research Institute, has stock options in Apogen Biotechnologies, Epic Bioscience, GRAIL, and has stock options and is co-founder of Achilles Therapeutics. Patents: C.S. holds European patents relating to assay technology to detect tumour recurrence (PCT/GB2017/053289); to targeting neoantigens (PCT/EP2016/059401), identifying patent response to immune checkpoint blockade (PCT/EP2016/071471), determining HLA LOH (PCT/GB2018/052004), predicting survival rates of patients with cancer (PCT/GB2020/050221), identifying patients who respond to cancer treatment (PCT/GB2018/051912), a US patent relating to detecting tumour mutations (PCT/US2017/28013) and both a European and US patent related to identifying insertion/deletion mutation targets (PCT/GB2018/051892). L.P. has received research funding from Pierre Fabre, and honoria from Pfizer, Ipsen, Bristol-Myers Squibb, and EUSA Pharma. S.B. has recieved institutional research funding from Astrazeneca, Tesaro, GSK; speakers fees from Amgen, Pfizer, Astrazeneca, Tesaro, GSK, Clovis, Takeda, Immunogen, Mersana and has an advisor role for Amgen, Astrazeneca, Epsilogen, Genmab, Immunogen, Mersana, MSD, Merck Serono, Oncxerna, Pfizer, Roche. W.C. has received honoraria from Janssen and AstraZeneca. Remaining authors have no conflicts of interest to declare.
Figures
References
-
- [cited 2021 20th July 2021];Confirmed cases of COVID-19 variants identified in UK. Latest updates on SARSCoV-2 variants detected in UK. 2021 16th July 2021. Available from: https://www.gov.uk/government/news/confirmed-cases-of-covid-19-variants-...2021.
-
- COVID-19: guidance on protecting people defined on medical grounds as extremely vulnerable. [cited 2021 20th July 2021];2021 Jul 20; Available from: https://www.gov.uk/government/publications/guidance-on-shielding-and-pro...2021.
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
- 18176/CRUK_/Cancer Research UK/United Kingdom
- 29911/CRUK_/Cancer Research UK/United Kingdom
- FC001988/CRUK_/Cancer Research UK/United Kingdom
- FC001002/WT_/Wellcome Trust/United Kingdom
- FC001169/WT_/Wellcome Trust/United Kingdom
- A18176/CRUK_/Cancer Research UK/United Kingdom
- FC001099/WT_/Wellcome Trust/United Kingdom
- FC001218/WT_/Wellcome Trust/United Kingdom
- FC001988/WT_/Wellcome Trust/United Kingdom
- FC001030/WT_/Wellcome Trust/United Kingdom
- FC001078/WT_/Wellcome Trust/United Kingdom
- FC011104/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
