

doi: 10.1186/s43019-021-00128-w.
Gait deviations of patients with ruptured anterior cruciate ligament: a cross-sectional gait analysis study on male patients
Affiliations
- PMID: 34952655
- PMCID: PMC8709949
- DOI: 10.1186/s43019-021-00128-w
Item in Clipboard
Gait deviations of patients with ruptured anterior cruciate ligament: a cross-sectional gait analysis study on male patients
Knee Surg Relat Res.
.
No abstract available
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
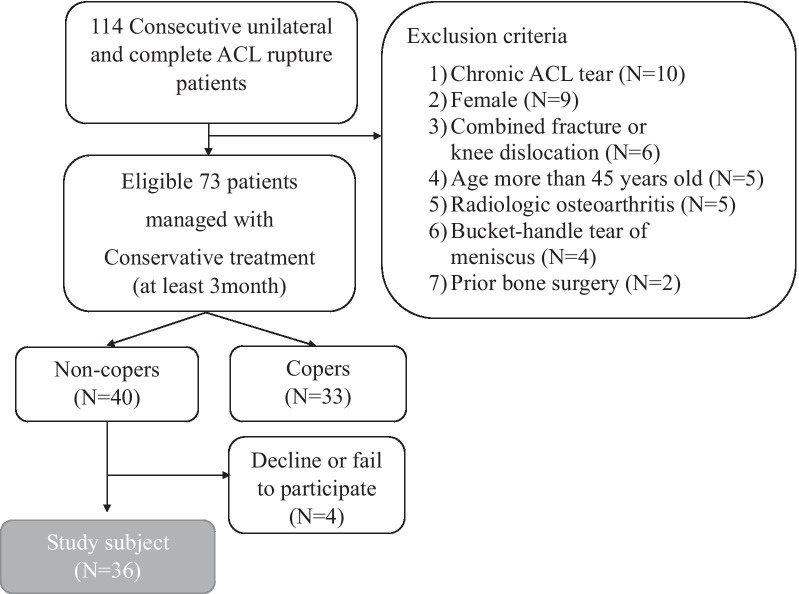
Study design and eligibility criteria. Thirty-six patients were included in this cross-sectional study
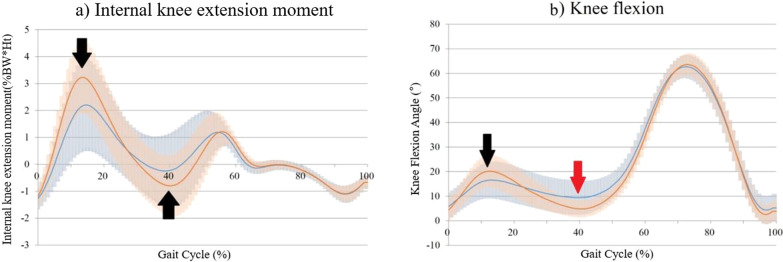
Kinetics and kinematics of the knee joint in the sagittal and axial planes. The blue curve indicates the ACL-ruptured limb, and the red curve indicates the contralateral uninjured limb. The shaded region represents mean ± one standard deviation. Table 1 presents a statistical analysis of the graph. a Knee extension moment. The knee extension moment peak value and amplitude were both smaller in the ACL-ruptured limb (black arrow). b Knee flexion angle. The ACL-ruptured knee showed extension at the IDS phase (black arrow) and more flexion from the SLS to the TDS phase (red arrow)

Schematic representations of knee extension moment (KEM) and knee flexion angle at the initial double-limb stance (IDS) phase. During this phase, ground reaction force (GRF) is generated for the repulsive body weight force (black arrow). The GRF can be divided into an axial vector (double arrow) and a transverse vector (dotted arrow). The axial vector runs parallel to the tibia and acts as a compressive force to the tibiofemoral joint. The transverse vector runs parallel to the ground and acts as a knee flexion force (counter to the knee extension moment by the quadriceps). The ACL-ruptured knee can be unstable during this phase, so patients try to reduce the transverse vector by extending their knee (note the difference in knee flexion angle). Instead, the tibiofemoral joint axial force can be increased. The graph shows the correlations between peak KEM and peak knee flexion at the IDS phase. The blue triangle represents the ACL-ruptured limb, and the orange circle represents the uninjured limb. Note the strong correlation between the two variables (Pearson r = 0.694, P < 0.001). Linear regression analysis showed that the adjusted R2 value of the first strategy was 0.475

Schematic representations of knee extension moment (KEM) and knee flexion angle during progression from the single-limb stance (SLS) to the terminal double-limb stance (TDS) phase. During this phase, the knee joint is more flexed in ACL-ruptured knees. Extended knees can be unstable during this phase because the KEM rapidly becomes negative (see the green KEM circle). Patients try to decrease the speed of the KEM changes by flexing their ACL-ruptured knee. This strategy has previously been described as the “quadriceps avoidance or stiffening strategy.” The lower right graph shows the correlation between KF PC3 (knee flexion principal component 2) and KEM PC2. KF PC3 represents the knee flexion angle during progression from the SLS to the TDS phase. KEM PC2 represents the KEM amplitude. The blue triangle represents the ACL-ruptured limb, and the orange circle represents the uninjured limb. Linear regression analysis showed that the adjusted R2 value of the second strategy was 0.497
References
LinkOut - more resources
Full Text Sources
