

Mobile stroke care expedites intravenous thrombolysis and endovascular thrombectomy
- PMID: 34952889
- PMCID: PMC9240459
- DOI: 10.1136/svn-2021-001119
Mobile stroke care expedites intravenous thrombolysis and endovascular thrombectomy
Abstract
Background: The number of mobile stroke programmes has increased with evidence, showing they expedite intravenous thrombolysis. Outstanding questions include whether time savings extend to patients eligible for endovascular therapy and impact clinical outcomes.
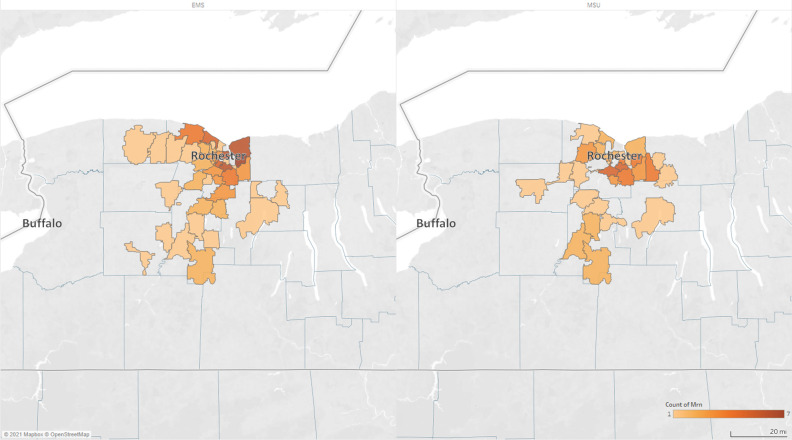
Objective: Our mobile stroke unit (MSU), based at an academic medical centre in upstate New York, launched in October 2018. We reviewed prospective observational data sets over 26 months to identify MSU and non-MSU emergency medical service (EMS) patients who underwent intravenous thrombolysis or endovascular thrombectomy for comparison of angiographic and clinical outcomes.
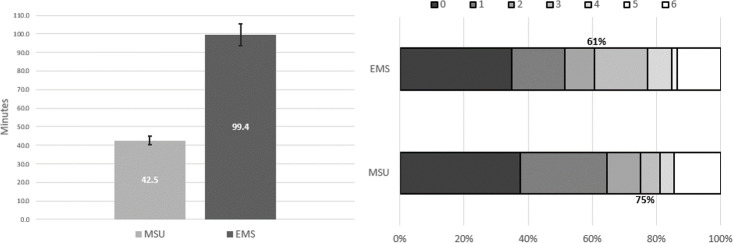
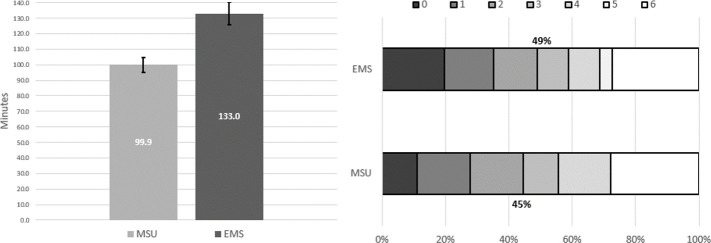
Results: Over 568 days in service, the MSU was dispatched 1489 times (2.6/day) and transported 300 patients (20% of dispatches). Intravenous tissue plasminogen activator (tPA) was administered to 57 MSU patients and the average time from 911 call-to-tPA was 42.5 min (±9.2), while EMS transported 73 patients who received tPA at 99.4 min (±35.7) (p<0.001). Seven MSU patients (12%) received tPA from 3.5 hours to 4.5 hours since last known well and would likely have been outside the window with EMS care. Endovascular thrombectomy was performed on 21 MSU patients with an average 911 call-to-groin puncture time of 99.9 min (±18.1), while EMS transported 54 patients who underwent endovascular thrombectomy (ET) at 133.0 min (±37.0) (p=0.0002). There was no difference between MSU and traditional EMS in modified Rankin score at 90-day clinic follow-up for patients undergoing intravenous thrombolysis or endovascular thrombectomy, whether assessed as a dichotomous or ordinal variable.
Conclusions: Mobile stroke care expedited both intravenous thrombolysis and endovascular thrombectomy. There is an ongoing need to show improved functional outcomes with MSU care.
Keywords: stroke; thrombectomy; thrombolytic therapy.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous