

Characteristics and prognosis of bloodstream infection in patients with COVID-19 admitted in the ICU: an ancillary study of the COVID-ICU study
- PMID: 34952960
- PMCID: PMC8708508
- DOI: 10.1186/s13613-021-00971-w
Characteristics and prognosis of bloodstream infection in patients with COVID-19 admitted in the ICU: an ancillary study of the COVID-ICU study
Erratum in
-
Correction to: Characteristics and prognosis of bloodstream infection in patients with COVID‑19 admitted in the ICU: an ancillary study of the COVID‑ICU study.Ann Intensive Care. 2022 Jan 11;12(1):4. doi: 10.1186/s13613-022-00979-w. Ann Intensive Care. 2022. PMID: 35015163 Free PMC article. No abstract available.
Abstract
Background: Patients infected with the severe acute respiratory syndrome coronavirus 2 (SARS-COV 2) and requiring intensive care unit (ICU) have a high incidence of hospital-acquired infections; however, data regarding hospital acquired bloodstream infections (BSI) are scarce. We aimed to investigate risk factors and outcome of BSI in critically ill coronavirus infectious disease-19 (COVID-19) patients.
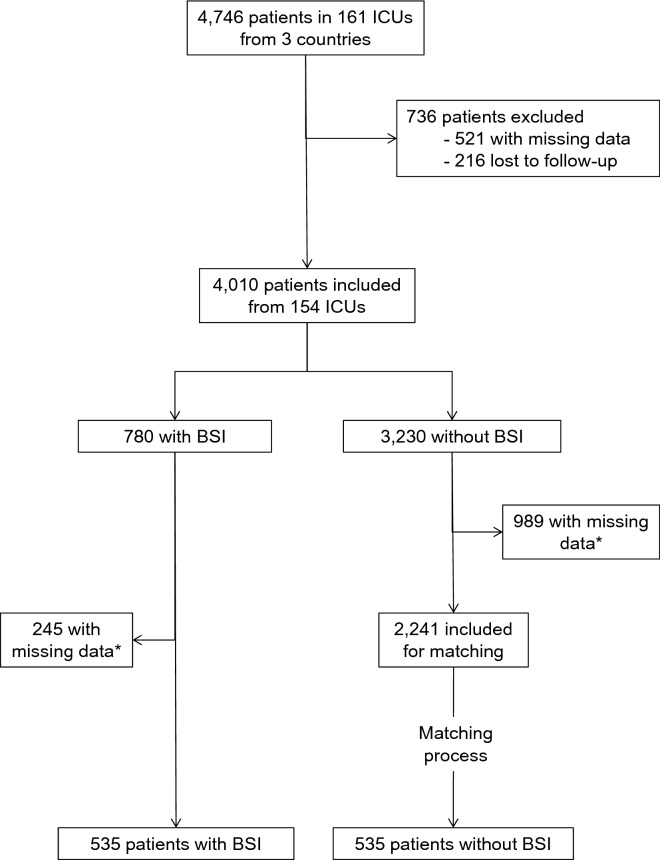
Patients and methods: We performed an ancillary analysis of a multicenter prospective international cohort study (COVID-ICU study) that included 4010 COVID-19 ICU patients. For the present analysis, only those with data regarding primary outcome (death within 90 days from admission) or BSI status were included. Risk factors for BSI were analyzed using Fine and Gray competing risk model. Then, for outcome comparison, 537 BSI-patients were matched with 537 controls using propensity score matching.
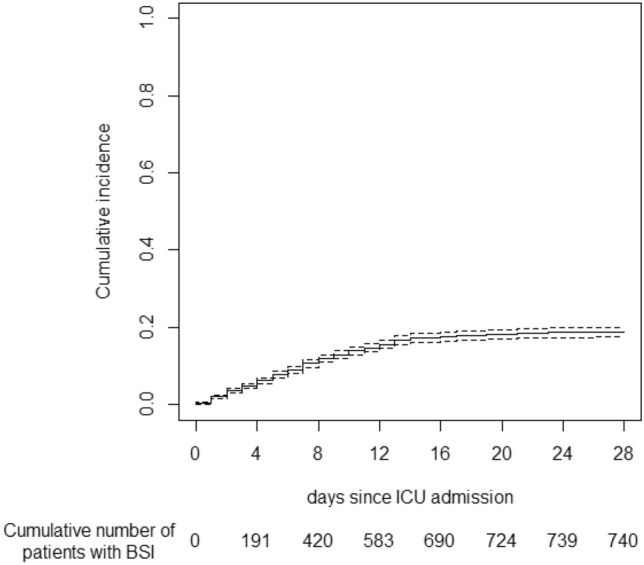
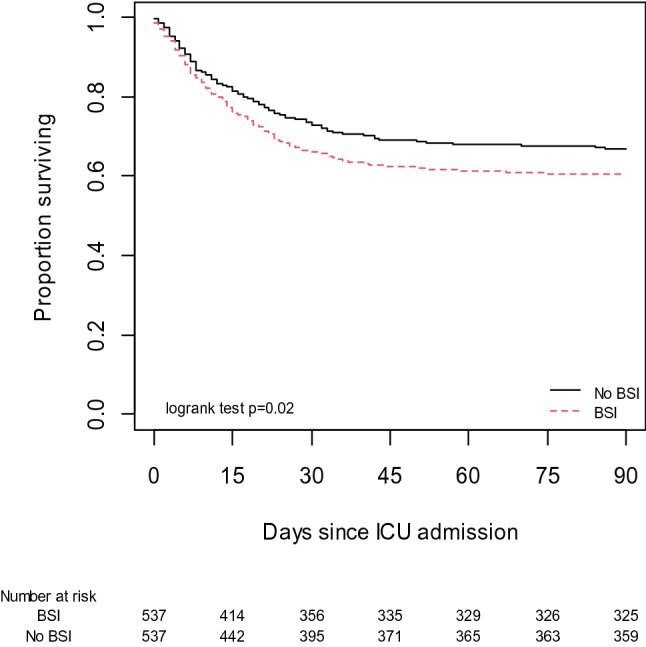
Results: Among 4010 included patients, 780 (19.5%) acquired a total of 1066 BSI (10.3 BSI per 1000 patients days at risk) of whom 92% were acquired in the ICU. Higher SAPS II, male gender, longer time from hospital to ICU admission and antiviral drug before admission were independently associated with an increased risk of BSI, and interestingly, this risk decreased over time. BSI was independently associated with a shorter time to death in the overall population (adjusted hazard ratio (aHR) 1.28, 95% CI 1.05-1.56) and, in the propensity score matched data set, patients with BSI had a higher mortality rate (39% vs 33% p = 0.036). BSI accounted for 3.6% of the death of the overall population.
Conclusion: COVID-19 ICU patients have a high risk of BSI, especially early after ICU admission, risk that increases with severity but not with corticosteroids use. BSI is associated with an increased mortality rate.
© 2021. The Author(s).
Conflict of interest statement
CEL has served as consultant for Bayer Healthcare, Carmat and Thermo Fisher Brahms, and received lecture fees from MSD, Aerogen and BioMérieux, outside the submitted work. The other authors have no conflicts of interest to declare in relationship to this manuscript.
Figures
References
-
- Luyt C-E, Sahnoun T, Gautier M, Vidal P, Burrel S, Pineton de Chambrun M, et al. Ventilator-associated pneumonia in patients with SARS-CoV-2-associated acute respiratory distress syndrome requiring ECMO: a retrospective cohort study. Ann Intensive Care. 2020;10:158. doi: 10.1186/s13613-020-00775-4. - DOI - PMC - PubMed
-
- Rouzé A, Martin-Loeches I, Povoa P, Makris D, Artigas A, Bouchereau M, et al. Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: a European multicenter cohort study. Intensive Care Med. 2021;47:188–198. doi: 10.1007/s00134-020-06323-9. - DOI - PMC - PubMed
-
- Razazi K, Arrestier R, Haudebourg AF, Benelli B, Carteaux G, Decousser J-W, et al. Risks of ventilator-associated pneumonia and invasive pulmonary aspergillosis in patients with viral acute respiratory distress syndrome related or not to Coronavirus 19 disease. Crit Care. 2020;24:699. doi: 10.1186/s13054-020-03417-0. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
