

Real-world application of tumor mutational burden-high (TMB-high) and microsatellite instability (MSI) confirms their utility as immunotherapy biomarkers
- PMID: 34953399
- PMCID: PMC8717431
- DOI: 10.1016/j.esmoop.2021.100336
Real-world application of tumor mutational burden-high (TMB-high) and microsatellite instability (MSI) confirms their utility as immunotherapy biomarkers
Abstract
Introduction: Microsatellite instability (MSI) testing and tumor mutational burden (TMB) are genomic biomarkers used to identify patients who are likely to benefit from immune checkpoint inhibitors. Pembrolizumab was recently approved by the Food and Drug Administration for use in TMB-high (TMB-H) tumors, regardless of histology, based on KEYNOTE-158. The primary objective of this retrospective study was real-world applicability and use of immunotherapy in TMB/MSI-high patients to lend credence to and refine this biomarker.
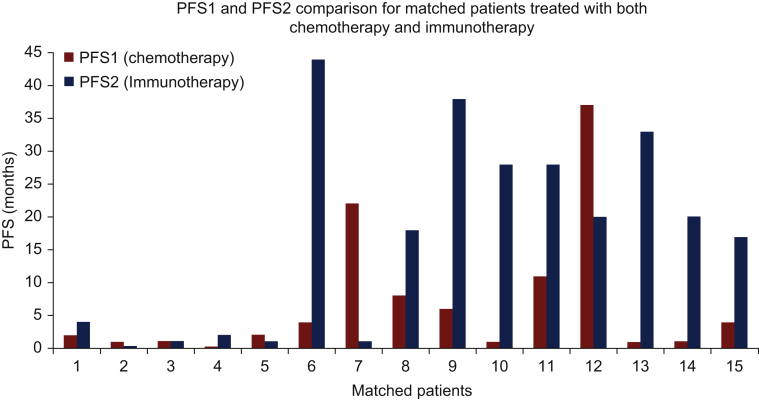
Methods: Charts of patients with advanced solid tumors who had MSI/TMB status determined by next generation sequencing (NGS) (FoundationOne CDx) were reviewed. Demographics, diagnosis, treatment history, and overall response rate (ORR) were abstracted. Progression-free survival (PFS) was determined from Kaplan-Meier curves. PFS1 (chemotherapy PFS) and PFS2 (immunotherapy PFS) were determined for patients who received immunotherapy after progressing on chemotherapy. The median PFS2/PFS1 ratio was recorded.
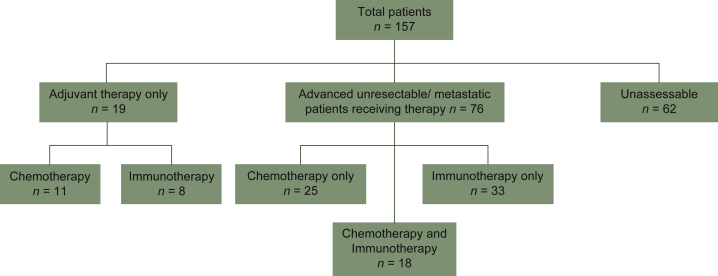
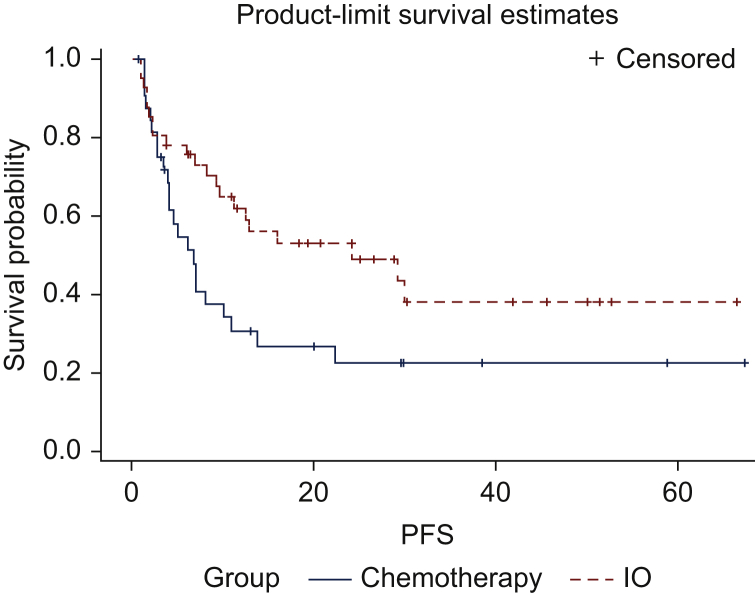
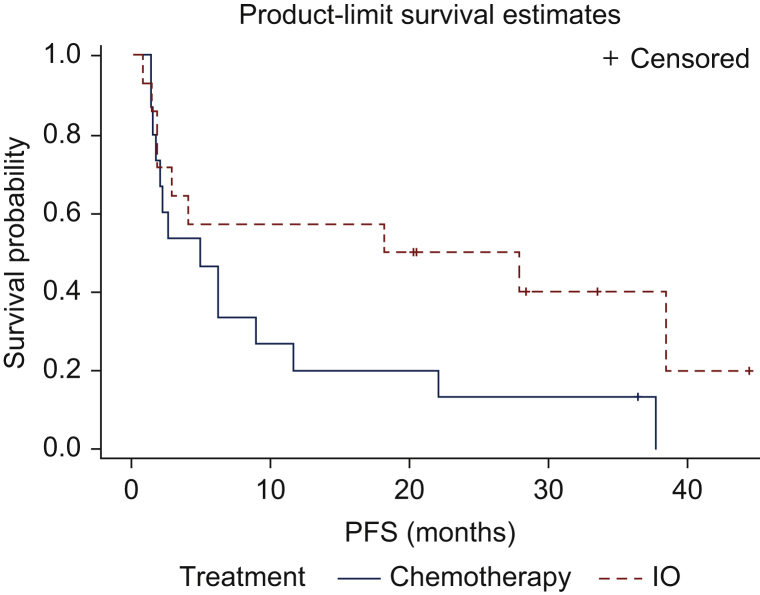
Results: MSI-high or TMB-H [≥20 mutations per megabase (mut/MB)] was detected in 157 adults with a total of 27 distinct tumor histologies. Median turnaround time for NGS was 73 days. ORR for most recent chemotherapy was 34.4%. ORR for immunotherapy was 55.9%. Median PFS for patients who received chemotherapy versus immunotherapy was 6.75 months (95% confidence interval, 3.9-10.9 months) and 24.2 months (95% confidence interval, 9.6 months to not reached), respectively (P = 0.042). Median PFS2/PFS1 ratio was 4.7 in favor of immunotherapy.
Conclusion: This real-world study reinforces the use of TMB as a predictive biomarker. Barriers exist to the timely implementation of NGS-based biomarkers and more data are needed to raise awareness about the clinical utility of TMB. Clinicians should consider treating TMB-H patients with immunotherapy regardless of their histology.
Keywords: biomarker; immune checkpoint inhibitors; microsatellite instability; precision medicine; tumor mutational burden.
Copyright © 2021. Published by Elsevier Ltd.
Conflict of interest statement
Disclosure TAC is a cofounder of Gritstone Oncology and own stock. TC has received funding from Bristol Myers Squibb (BMS), AstraZeneca, Illumina, NysnoBio, Pfizer. VS reports grants from LOXO Oncology during the conduct of the study and Bayer outside the submitted work, and research funding/grant support for clinical trials (to his institution) from AbbVie, Agensys, Alfa-153 sigma, Altum, Amgen, Bayer, Berg Health, Blueprint, Boston Biomedical, Boston Pharmaceuticals, D3, Dragonfly Therapeutics, Exelixis, Fujifilm, Idera Pharma, Incyte, InhibRx, Loxo Oncology, Medimmune, MultiVir, NCI Cancer, Therapy Evaluation Program, National Comprehensive Cancer Network, Novartis, PharmaMar, Pfizer, Takeda, Turning Point Therapeutics, and University of Texas MD Anderson Cancer Center. RG reports research funding/grant support for clinical trials (to his institution) from Regeneron, BMS, Merck/EMD Serano, Amgen, Roche/Genentech, Philogen. Consulting/advisory board from Regeneron. Speaker for Deciphera. Currently employee of Merck. This manuscript and all work pertaining to it was done prior to employment at Merck. All other authors have declared no conflicts of interest.
Figures
References
-
- Rizvi H., Sanchez-Vega F., La K., et al. Molecular determinants of response to anti-programmed cell death (PD)-1 and anti-programmed death-ligand 1 (PD-L1) blockade in patients with non-small-cell lung cancer profiled with targeted next-generation sequencing. J Clin Oncol. 2018;36(7):633–641. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
