

Efficacy and safety of two neutralising monoclonal antibody therapies, sotrovimab and BRII-196 plus BRII-198, for adults hospitalised with COVID-19 (TICO): a randomised controlled trial
- PMID: 34953520
- PMCID: PMC8700279
- DOI: 10.1016/S1473-3099(21)00751-9
Efficacy and safety of two neutralising monoclonal antibody therapies, sotrovimab and BRII-196 plus BRII-198, for adults hospitalised with COVID-19 (TICO): a randomised controlled trial
Abstract
Background: We aimed to assess the efficacy and safety of two neutralising monoclonal antibody therapies (sotrovimab [Vir Biotechnology and GlaxoSmithKline] and BRII-196 plus BRII-198 [Brii Biosciences]) for adults admitted to hospital for COVID-19 (hereafter referred to as hospitalised) with COVID-19.
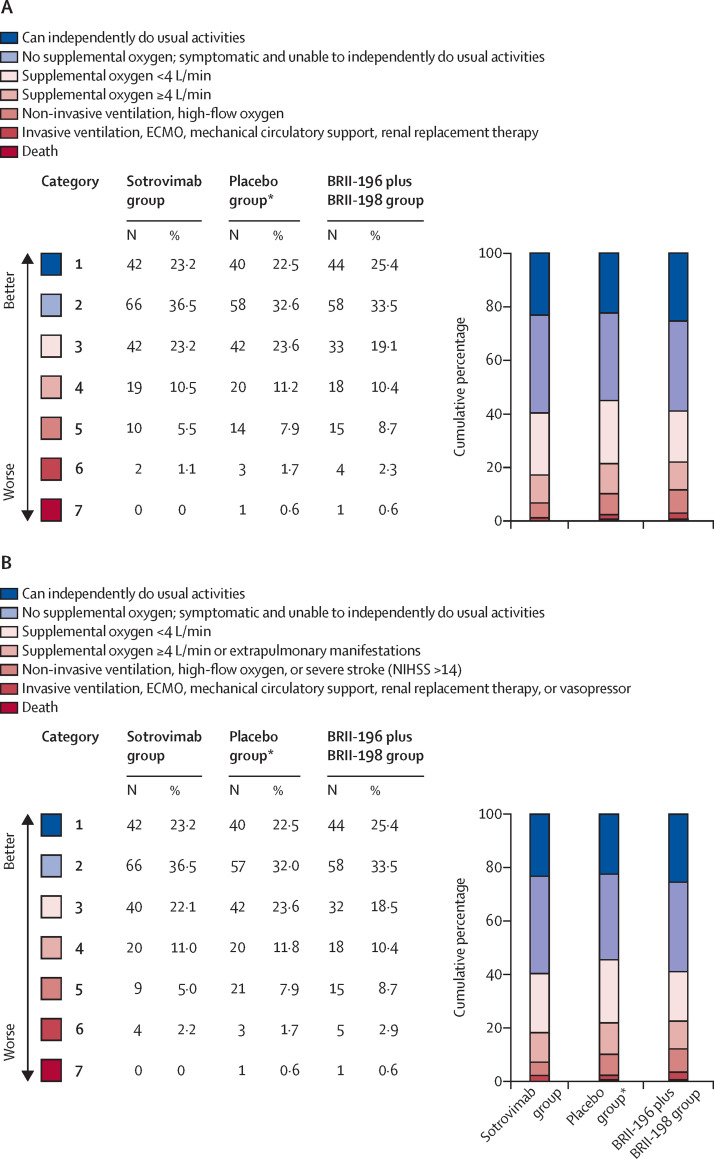
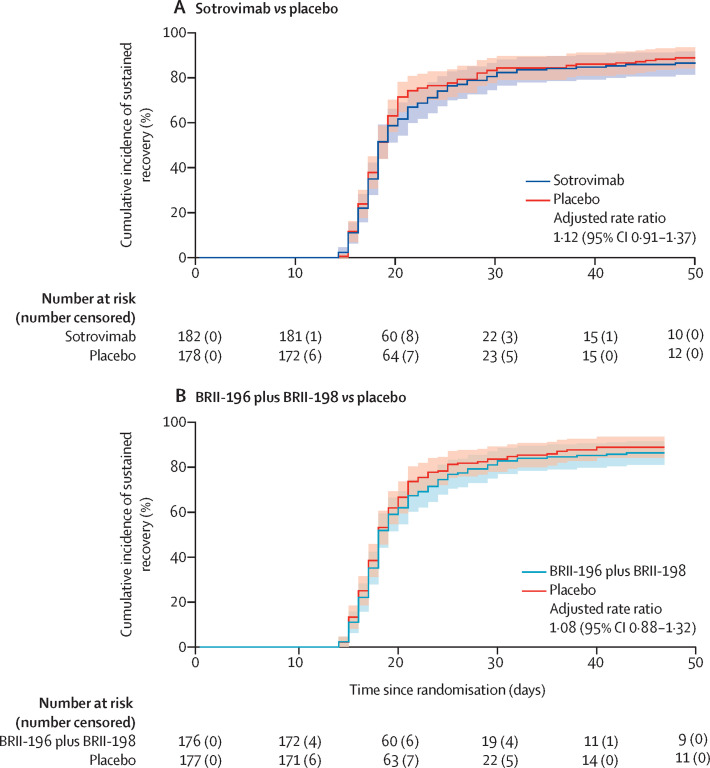
Methods: In this multinational, double-blind, randomised, placebo-controlled, clinical trial (Therapeutics for Inpatients with COVID-19 [TICO]), adults (aged ≥18 years) hospitalised with COVID-19 at 43 hospitals in the USA, Denmark, Switzerland, and Poland were recruited. Patients were eligible if they had laboratory-confirmed SARS-CoV-2 infection and COVID-19 symptoms for up to 12 days. Using a web-based application, participants were randomly assigned (2:1:2:1), stratified by trial site pharmacy, to sotrovimab 500 mg, matching placebo for sotrovimab, BRII-196 1000 mg plus BRII-198 1000 mg, or matching placebo for BRII-196 plus BRII-198, in addition to standard of care. Each study product was administered as a single dose given intravenously over 60 min. The concurrent placebo groups were pooled for analyses. The primary outcome was time to sustained clinical recovery, defined as discharge from the hospital to home and remaining at home for 14 consecutive days, up to day 90 after randomisation. Interim futility analyses were based on two seven-category ordinal outcome scales on day 5 that measured pulmonary status and extrapulmonary complications of COVID-19. The safety outcome was a composite of death, serious adverse events, incident organ failure, and serious coinfection up to day 90 after randomisation. Efficacy and safety outcomes were assessed in the modified intention-to-treat population, defined as all patients randomly assigned to treatment who started the study infusion. This study is registered with ClinicalTrials.gov, NCT04501978.
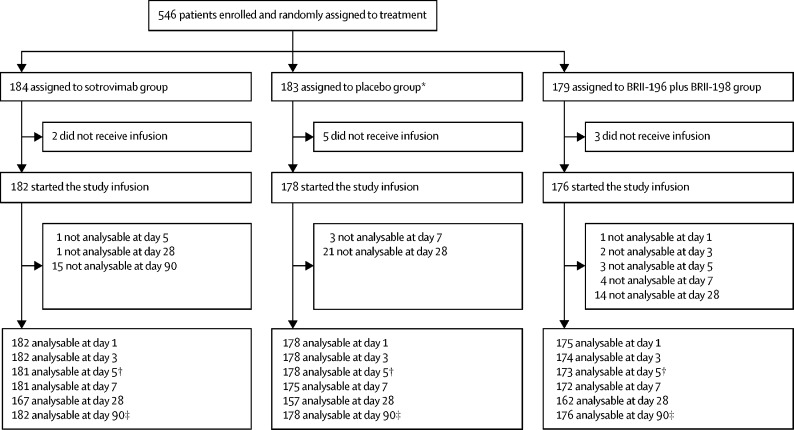
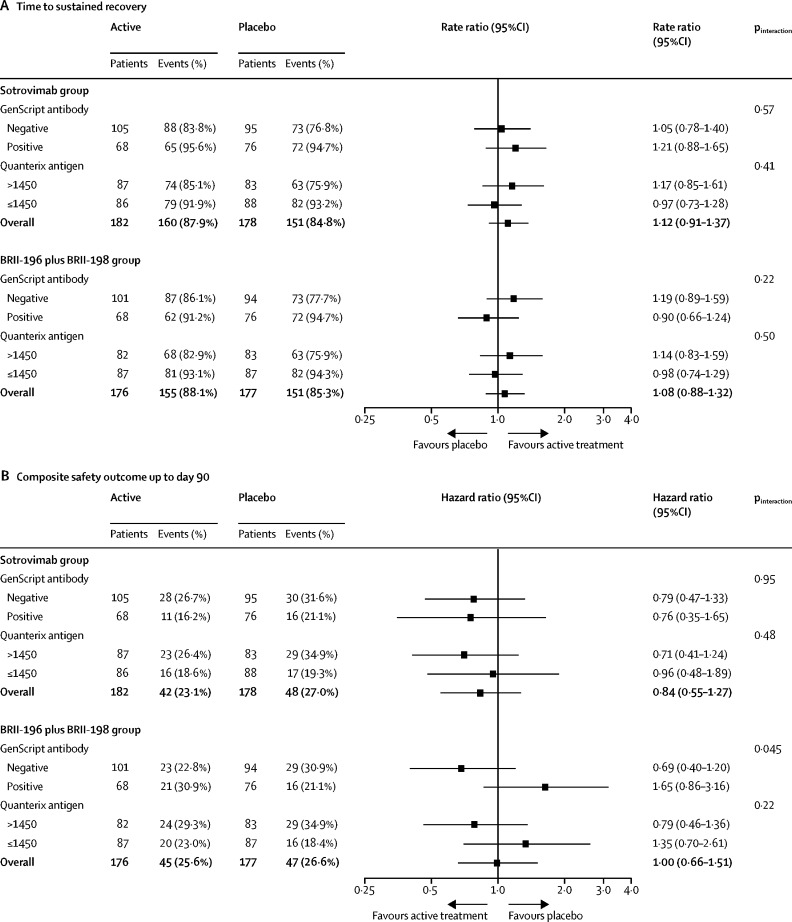
Findings: Between Dec 16, 2020, and March 1, 2021, 546 patients were enrolled and randomly assigned to sotrovimab (n=184), BRII-196 plus BRII-198 (n=183), or placebo (n=179), of whom 536 received part or all of their assigned study drug (sotrovimab n=182, BRII-196 plus BRII-198 n=176, or placebo n=178; median age of 60 years [IQR 50-72], 228 [43%] patients were female and 308 [57%] were male). At this point, enrolment was halted on the basis of the interim futility analysis. At day 5, neither the sotrovimab group nor the BRII-196 plus BRII-198 group had significantly higher odds of more favourable outcomes than the placebo group on either the pulmonary scale (adjusted odds ratio sotrovimab 1·07 [95% CI 0·74-1·56]; BRII-196 plus BRII-198 0·98 [95% CI 0·67-1·43]) or the pulmonary-plus complications scale (sotrovimab 1·08 [0·74-1·58]; BRII-196 plus BRII-198 1·00 [0·68-1·46]). By day 90, sustained clinical recovery was seen in 151 (85%) patients in the placebo group compared with 160 (88%) in the sotrovimab group (adjusted rate ratio 1·12 [95% CI 0·91-1·37]) and 155 (88%) in the BRII-196 plus BRII-198 group (1·08 [0·88-1·32]). The composite safety outcome up to day 90 was met by 48 (27%) patients in the placebo group, 42 (23%) in the sotrovimab group, and 45 (26%) in the BRII-196 plus BRII-198 group. 13 (7%) patients in the placebo group, 14 (8%) in the sotrovimab group, and 15 (9%) in the BRII-196 plus BRII-198 group died up to day 90.
Interpretation: Neither sotrovimab nor BRII-196 plus BRII-198 showed efficacy for improving clinical outcomes among adults hospitalised with COVID-19.
Funding: US National Institutes of Health and Operation Warp Speed.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests WHS reports grants from National Heart, Lung and Blood Institute (NHLBI) during the conduct of the study and personal fees from Aerpio Pharmaceuticals outside of the submitted work. US reports grants from NIH, Cytodin, and Regeneron outside of the submitted work. RLG reports personal fees from GSK Pharmaceuticals during the conduct of the study, and personal fees and non-financial support from Gilead Sciences and personal fees from Johnson & Johnson and Roivant Sciences, outside of the submitted work. TWR reports grants from NHLBI of the NIH during the conduct of the study and personal fees from Cumberland Pharmaceuticals and Sanofi outside of the submitted work. JDC reports grants from NIH outside the submitted work. IDP reports grants from NIH during the conduct of the study, and grants from Janssen Pharmaceuticals, NIH, and US Centers for Disease Control and Prevention (CDC), research funding support from Regeneron and Asahi Kasei Pharma, and grants from Intermountain Research and Medical Foundation outside the submitted work. AJR reports personal fees from Merck outside of the submitted work. MNG reports research funding support from Regeneron outside of the submitted work. BWT reports salary support from INSIGHT during the conduct of the study, and grants from NIH, Agency for Healthcare Research and Quality, CDC, Veterans Affairs Health Services Research and Development, grants and personal fees from Zambon pharmaceuticals, and personal fees and research funding support from Genentech outside of the submitted work. MKJ reports payment to their employer for clinical trial activities from Regeneron Pharmaceuticals, Gilead Sciences, Janssen Pharmaceuticals, and Merck, and payments for advisory board meetings from Gilead Sciences outside of the submitted work. AK reports grants from United Therapeutics, Johnson & Johnson, 4D Medical, Lung LLC, and Reata Pharmaceuticals outside of the submitted work. MAM reports grants from Roche/Genentec and personal fees from Pliant Therapeutics, Novartis, Johnson & Johnson, and Citius Pharmaceuticals outside of the submitted work. AAG reports grants from NIH during the conduct of the study and grants from AbbVie and Faron Pharmaceuticals outside of the submitted work. SMB reports grants from CDC during the conduct of the study and personal fees from Hamilton, payment to their employer for service on a trial steering committee from Faron and Sedana; grants from Janssen, NIH, and US Department of Defense; and book royalties from Oxford University and Brigham Young University outside of the submitted work. SP reports grants to their university from the University of Minnesota during the conduct of the study, and other grants to their university from University of Minnesota, European and Developing Countries Clinical Trials Partnership, UK Research and Innovation (UKRI), Academy of Medical Sciences, ViiV Healthcare, UK Medical Research Council (MRC), and Gilead Sciences outside of the submitted work. HFG reports grants from Swiss National Science Foundation, NIH, Swiss HIV Cohort Study, and Yvonne Jacob Foundation; unrestricted grants from Gilead Sciences; and personal fees from Merck, Gilead Sciences and ViiV, for being an advisor, consultant, or DSMB member, outside of the submitted work. SS reports grants from NIH during the conduct of the study. HC reports being a Gilead employee. RG reports being a full-time employee of Vir Biotechnology and owned stock in Vir Biotechnology during the conduct of the study. SO reports being an employee of GlaxoSmithKline Pharmaceuticals. DM reports support from Brii Biosciences during the conduct of the study. AGB reports grants from University of Minnesota during the conduct of the study and grants from MRC and UKRI outside of the submitted work. BTT reports receiving consulting fees from Bayer, Novartis, and Thetis outside the submitted work. JDN reports grants from NIAID NIH during the conduct of the study. All other members of the writing committee declare no competing interests.
Figures
Comment in
-
Time to knock monoclonal antibodies off the platform for patients hospitalised with COVID-19.Lancet Infect Dis. 2022 May;22(5):567-569. doi: 10.1016/S1473-3099(21)00762-3. Epub 2021 Dec 23. Lancet Infect Dis. 2022. PMID: 34953521 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 TR002541/TR/NCATS NIH HHS/United States
- U01 HL088942/HL/NHLBI NIH HHS/United States
- K08 AI141761/AI/NIAID NIH HHS/United States
- MRC_UU_12023/23/MRC_/Medical Research Council/United Kingdom
- UL1 TR003015/TR/NCATS NIH HHS/United States
- T32 GM135169/GM/NIGMS NIH HHS/United States
- K23 GM129661/GM/NIGMS NIH HHS/United States
- MC_UU_00004/04/MRC_/Medical Research Council/United Kingdom
- T32 HL069749/HL/NHLBI NIH HHS/United States
- UL1 TR001102/TR/NCATS NIH HHS/United States
- K23 HL153584/HL/NHLBI NIH HHS/United States
- OT2 HL156812/HL/NHLBI NIH HHS/United States
- KL2 TR003016/TR/NCATS NIH HHS/United States
- UM1 HL117924/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
