

Antibiotic prophylaxis in preterm premature rupture of membranes at 24-31 weeks' gestation: Perinatal and 2-year outcomes in the EPIPAGE-2 cohort
- PMID: 34954867
- PMCID: PMC9546066
- DOI: 10.1111/1471-0528.17081
Antibiotic prophylaxis in preterm premature rupture of membranes at 24-31 weeks' gestation: Perinatal and 2-year outcomes in the EPIPAGE-2 cohort
Abstract
Objective: To compare different antibiotic prophylaxis administered after preterm premature rupture of membranes to determine whether any were associated with differences in obstetric and/or neonatal outcomes and/or neurodevelopmental outcomes at 2 years of corrected age.
Design: Prospective, nationwide, population-based EPIPAGE-2 cohort study of preterm infants.
Setting: France, 2011.
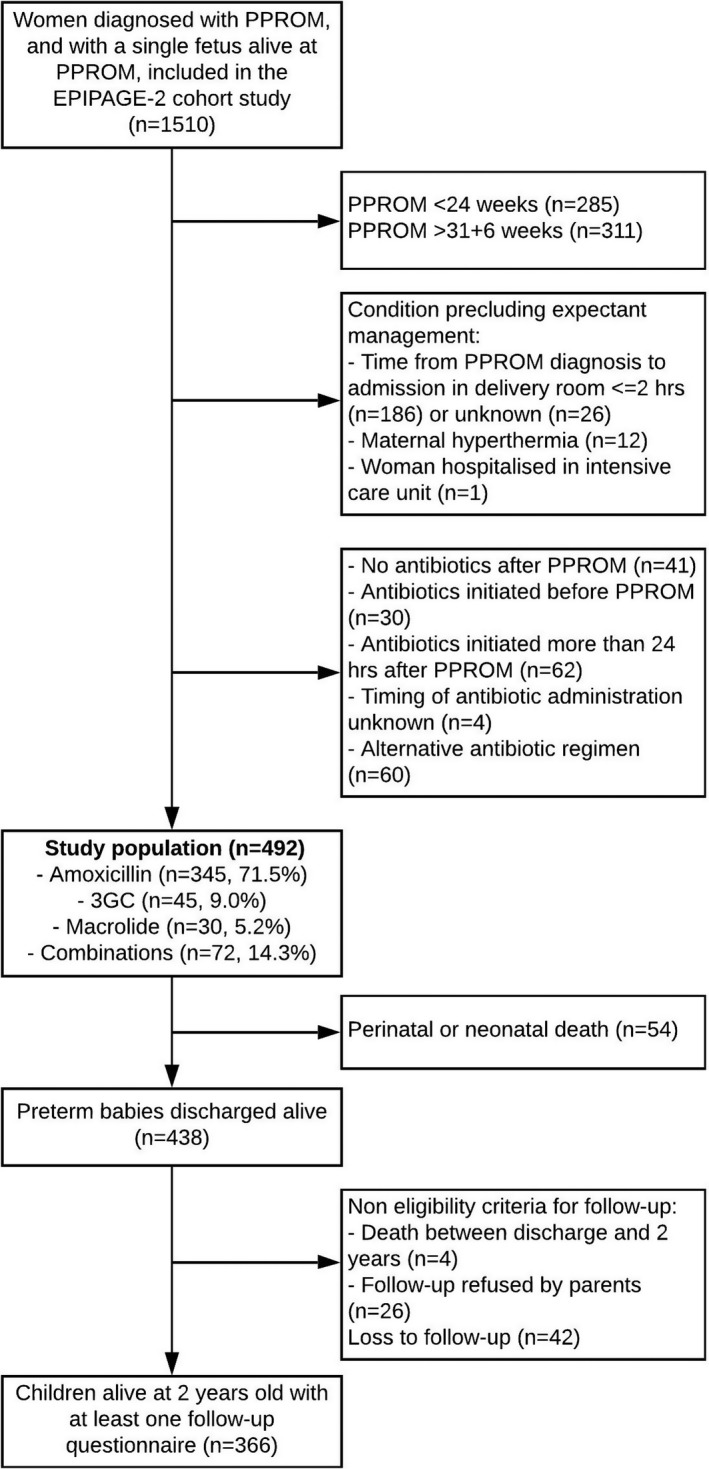
Sample: We included 492 women with a singleton pregnancy and a diagnosis of preterm premature rupture of membranes at 24-31 weeks. Exclusion criteria were contraindication to expectant management or indication for antibiotic therapy other than preterm premature rupture of membranes. Antibiotic prophylaxis was categorised as amoxicillin (n = 345), macrolide (n = 30), third-generation cephalosporin (n = 45) or any combinations covering Streptococcus agalactiae and >90% of Escherichia coli (n = 72), initiated within 24 hours after preterm premature rupture of membranes.
Methods: Population-averaged robust Poisson models.
Main outcome measures: Survival at discharge without severe neonatal morbidity, 2-year neurodevelopment.
Results: With amoxicillin, macrolide, third-generation cephalosporin and combinations, 78.5%, 83.9%, 93.6% and 86.0% of neonates were discharged alive without severe morbidity. The administration of third-generation cephalosporin or any E. coli-targeting combinations was associated with improved survival without severe morbidity (adjusted risk ratio 1.25 [95% confidence interval 1.08-1.45] and 1.10 [95 % confidence interval 1.01-1.20], respectively) compared with amoxicillin. We evidenced no increase in neonatal sepsis related to third-generation cephalosporin-resistant pathogen.
Conclusion: In preterm premature rupture of membranes at 24-31 weeks, antibiotic prophylaxis based on third-generation cephalosporin may be associated with improved survival without severe neonatal morbidity when compared with amoxicillin, with no evidence of increase in neonatal sepsis related to third-generation cephalosporin-resistant pathogen.
Tweetable abstract: Antibiotic prophylaxis after PPROM at 24-31 weeks: 3rd-generation cephalosporins associated with improved neonatal outcomes.
Keywords: amoxicillin; antenatal management; cephalosporins; latency; macrolides; neurodevelopment; obstetric intervention; perinatal outcome; prematurity; prophylactic antibiotics.
© 2022 The Authors. BJOG: An International Journal of Obstetrics and Gynaecology published by John Wiley & Sons Ltd.
Conflict of interest statement
None declared. Completed disclosure of interest forms are available to view online as supporting information.
Figures
References
-
- Mercer BM. Preterm premature rupture of the membranes. Obstet Gynecol. 2003;101(1):178–93. - PubMed
-
- Schmitz T, Sentilhes L, Lorthe E, Gallot D, Madar H, Doret‐Dion M, et al. Preterm premature rupture of the membranes: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians (CNGOF). Eur J Obstet Gynecol Reprod Biol. 2019;236:1–6. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
