

Imaging update in spinal tuberculosis
- PMID: 34956831
- PMCID: PMC8671643
- DOI: 10.1016/j.jcot.2021.101742
Imaging update in spinal tuberculosis
Abstract
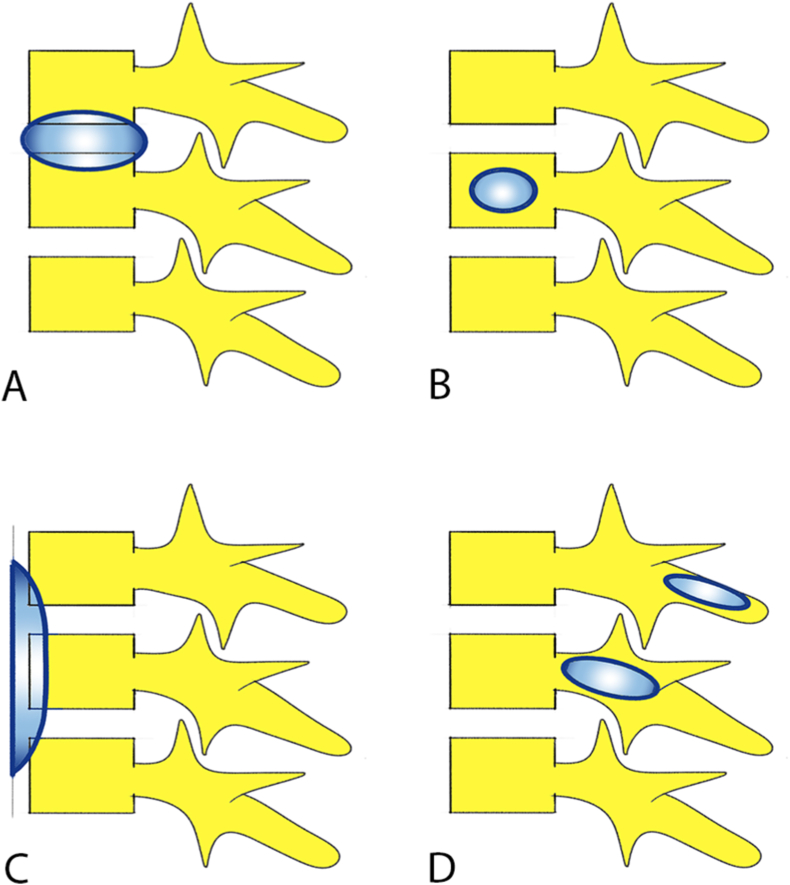
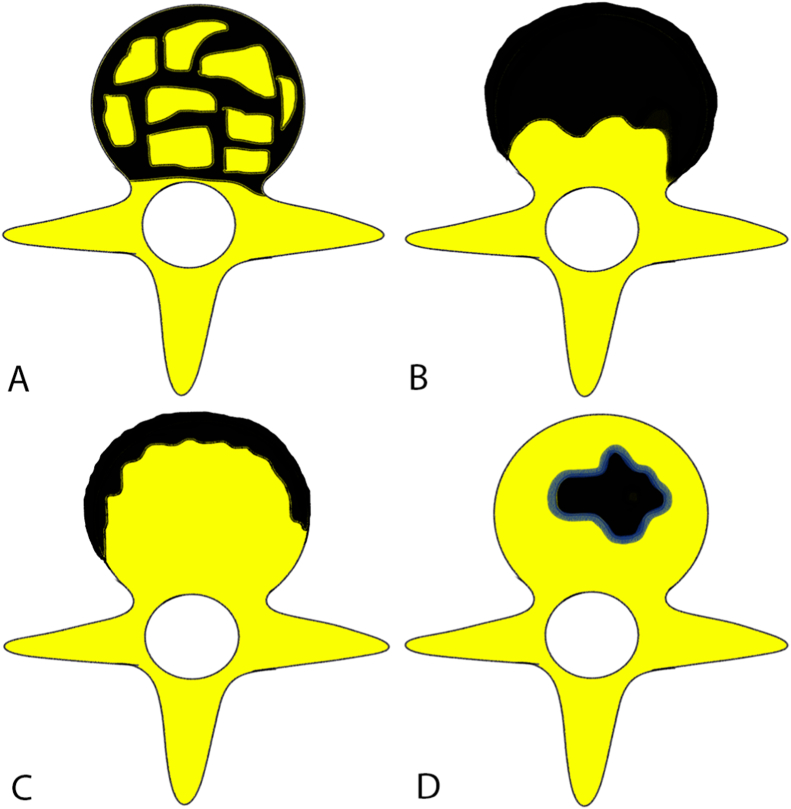
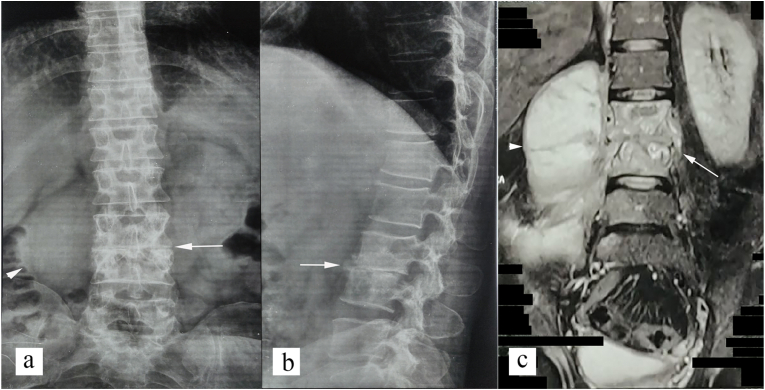
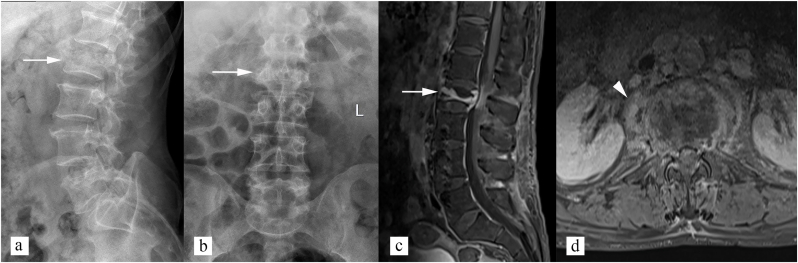
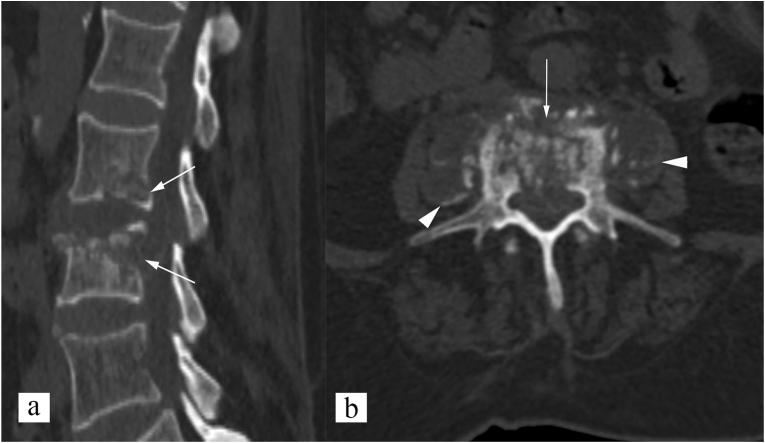
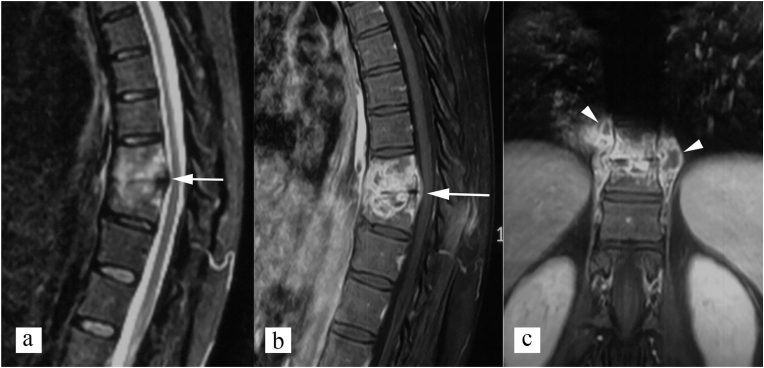
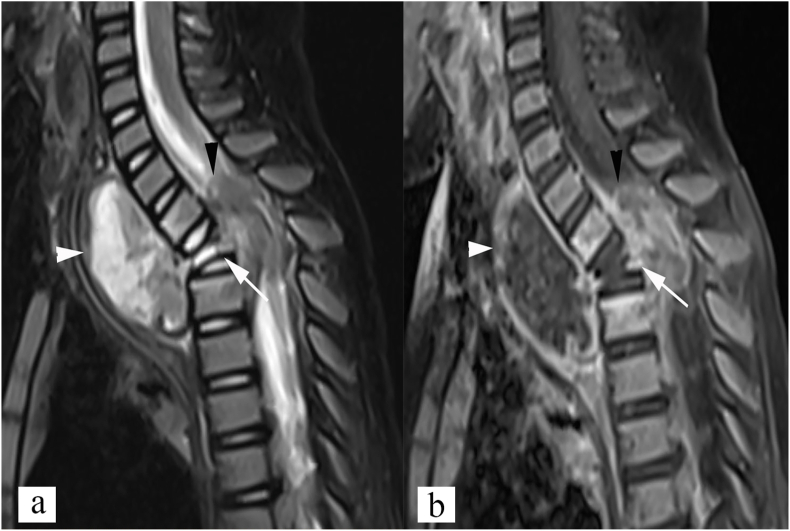
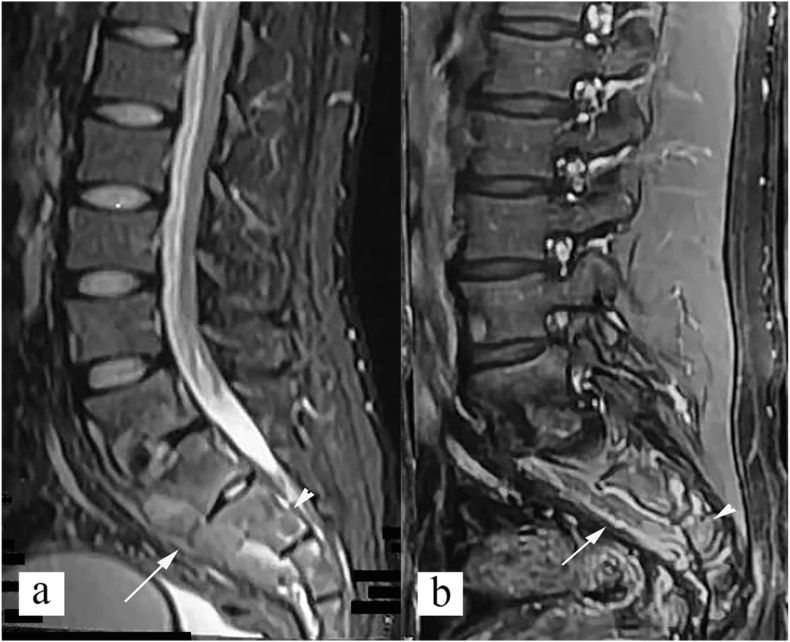
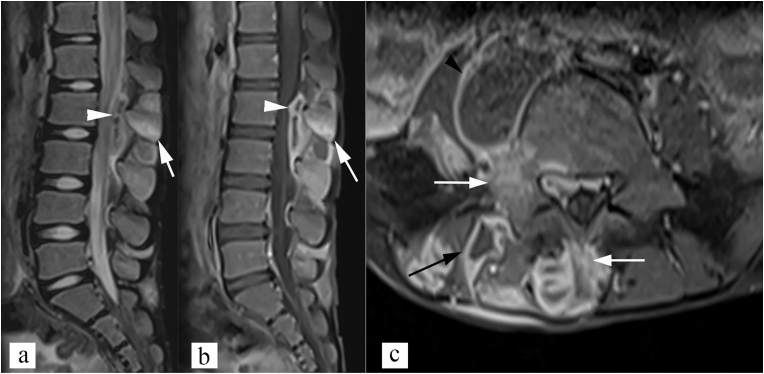
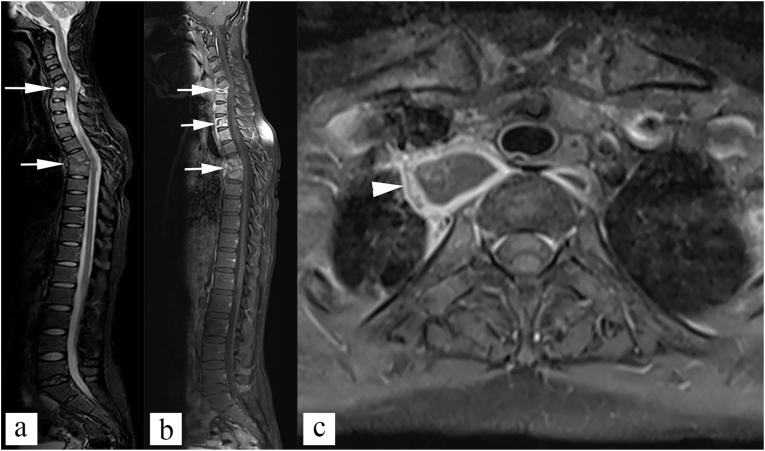
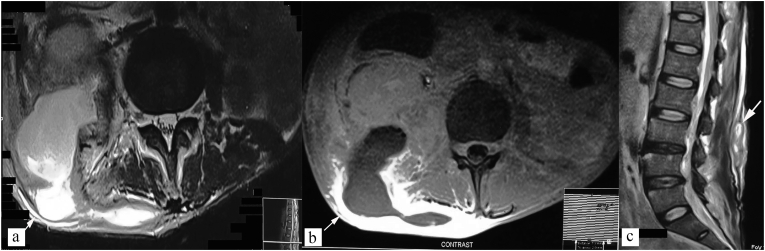
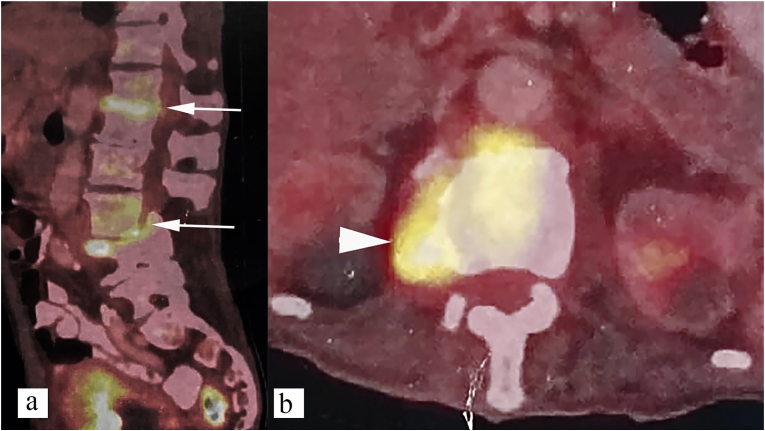
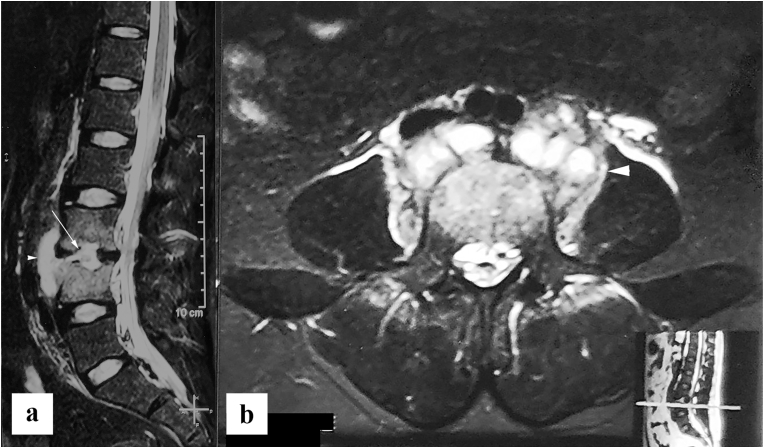
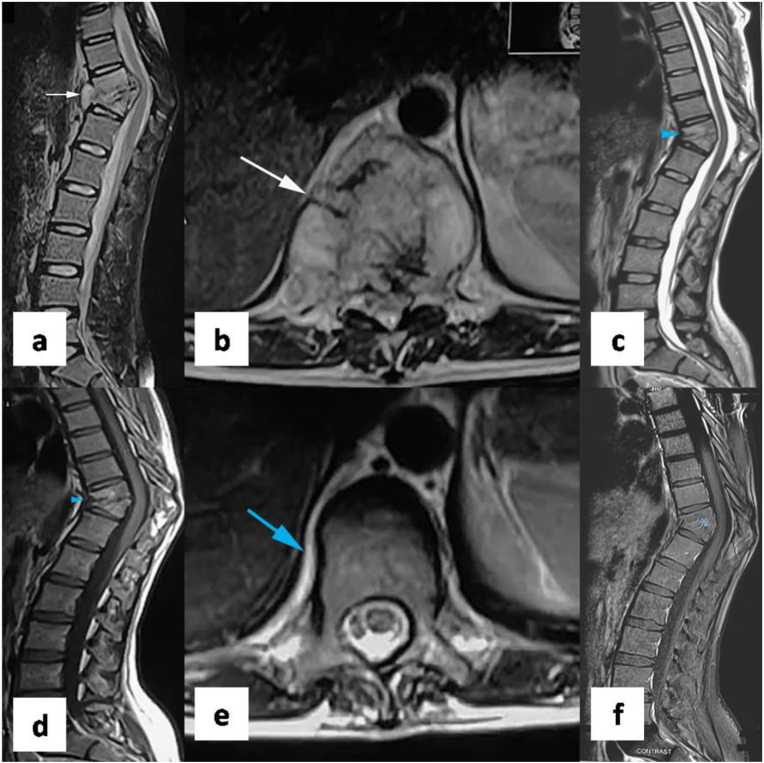
Tuberculosis is ancient disease known to mankind. Diagnosis and management of spinal tuberculosis has immensely improved in last few decades. Imaging, particularly MRI, plays important role in diagnosis of spinal tuberculosis and its complications. Four common imaging patterns of spinal tuberculosis include paradiscal type, central type, Anterior subligamentous type, and posterior type. Imaging also plays important role in differentiation of spinal tuberculosis from its mimics, particularly pyogenic spondylitis, and metastasis. Radiological interventions, such as CT guided vertebral biopsy, and percutaneous drainage of cold abscess, are commonly used in management of spinal tuberculosis. Monitoring of therapeutic response is often based on clinical evaluation and imaging. MRI is most common imaging modality used. Signs of healing include bony ankylosis, resolution of marrow edema, decrease in contrast enhancement, and fatty change with in bone marrow. PET CT is recently evaluated for response assessment with promising results. This review summarizes pathophysiology, clinical presentation, imaging features, radiological interventions, and response assessment in spinal tuberculosis.
Keywords: Imaging intervention; Response evaluation; Spinal infection imaging; Spinal tuberculosis.
© 2021.
Conflict of interest statement
None.
Figures

References
-
- Duraiswami P.K., Orth M., Tuli S.M. 5000 years of orthopaedics in India. Clin Orthop. 1971 Apr;75:269–280. PMID: 4929008. - PubMed
Publication types
LinkOut - more resources
Full Text Sources