

Agreement and Repeatability of Central and Peripheral Refraction by One Novel Multispectral-Based Refractor
- PMID: 34957151
- PMCID: PMC8695908
- DOI: 10.3389/fmed.2021.777685
Agreement and Repeatability of Central and Peripheral Refraction by One Novel Multispectral-Based Refractor
Abstract
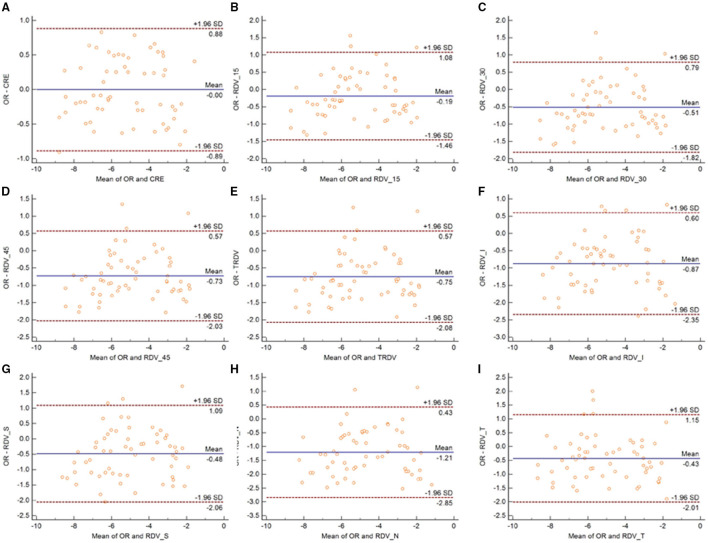
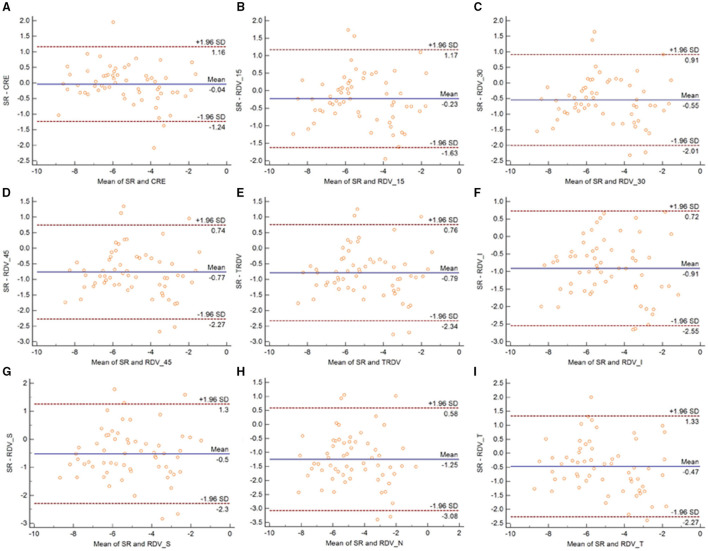
Purpose: To evaluate the repeatability of a multispectral-based refractor in central and peripheral refraction measurement, and to assess the agreement of such measurements with objective refraction (OR) and subjective refraction (SR) in patients with myopia. Methods: A total of 60 subjects were recruited in this prospective research. Patients were divided into three groups according to the refractive error. Next, the central and peripheral refraction parameters were measured using multispectral refractive tomography (MRT) before and after cycloplegia. In addition, OR and SR measurements were also performed. The intraobserver repeatability was analyzed using within-subject standard deviation (Sw), test-retest repeatability (TRT), and intraclass correlation coefficient (ICC). Agreement was evaluated using Bland-Altman plot and 95% limits of agreement (LoA). Results: The ICC value of central and peripheral refraction were all higher than 0.97 with or without cycloplegia. The peripheral refraction in the nasal, temporal, superior, and inferior quadrants was slightly worse than other parameters, with the largest error interval being 1.43 D. The 95% LoA of the central refraction and OR or SR ranged from -0.89 to 0.88 D and -1.24 to 1.16 D without cycloplegia, respectively, and from -0.80 to 0.42 D and -1.39 to -0.84 D under cycloplegia, respectively. Conclusions: The novel multispectral refraction topography demonstrated good repeatability in central and peripheral refraction. However, the refraction in the nasal, temporal, superior, and inferior quadrants were not as good as that of central and circle peripheral refraction.
Keywords: agreement; myopia; ophthalmology; refraction; repeatability.
Copyright © 2021 Lu, Ji, Ding, Tian, Long, Guo and Leng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources
Research Materials