

Effectiveness of rosuvastatin plus colchicine, emtricitabine/tenofovir and combinations thereof in hospitalized patients with COVID-19: a pragmatic, open-label randomized trial
- PMID: 34957385
- PMCID: PMC8686571
- DOI: 10.1016/j.eclinm.2021.101242
Effectiveness of rosuvastatin plus colchicine, emtricitabine/tenofovir and combinations thereof in hospitalized patients with COVID-19: a pragmatic, open-label randomized trial
Abstract
Background: The use of rosuvastatin plus colchicine and emtricitabine/tenofovir in hospitalized patients with SARS-CoV-2 disease (COVID-19) has not been assessed. The objective of this study was to assess the effectiveness and safety of rosuvastatin plus colchicine, emtricitabine/tenofovir, and their combined use in these patients.
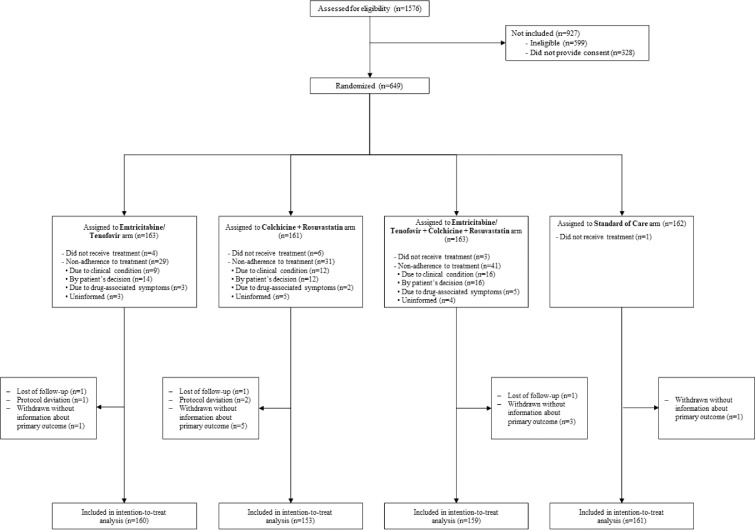
Methods: This was a randomized, controlled, open-label, multicentre, parallel, pragmatic study conducted in six referral hospitals in Bogotá, Colombia. The study enrolled hospitalized patients over 18 years of age with a confirmed diagnosis of COVID-19 complicated with pneumonia, not on chronic treatment with the study medications, and with no contraindications for their use. Patients were assigned 1:1:1:1. 1) emtricitabine with tenofovir disoproxil fumarate (FTC/TDF, 200/300 mg given orally for 10 days); 2) colchicine plus rosuvastatin (COLCH+ROSU, 0.5 mg and 40 mg given orally for 14 days); 3) emtricitabine with tenofovir disoproxil plus colchicine and rosuvastatin at the same doses and for the same period of time (FTC/TDF+COLCH+ROSU); or 4) the Colombian consensus standard of care, including a corticosteroid (SOC). The primary endpoint was 28-day all-cause mortality. A modified intention-to-treat analysis was used together with a usefulness analysis to determine which could be the best treatment. The trial was registered at ClinicalTrials.gov: NCT04359095.
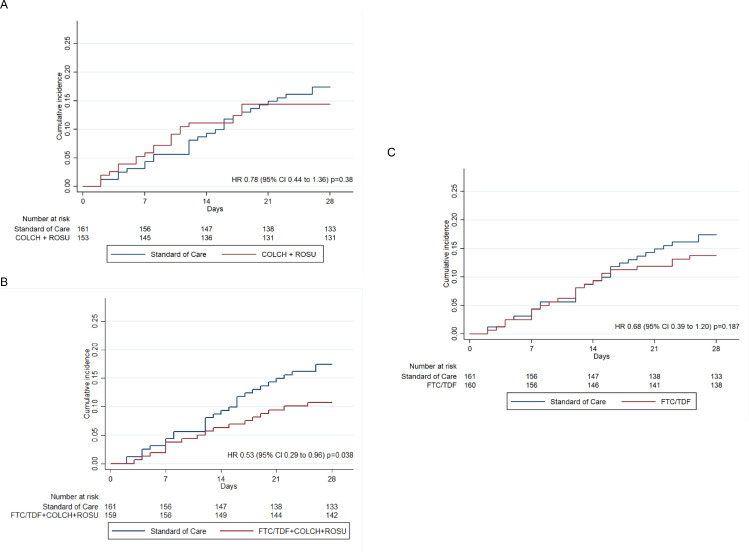
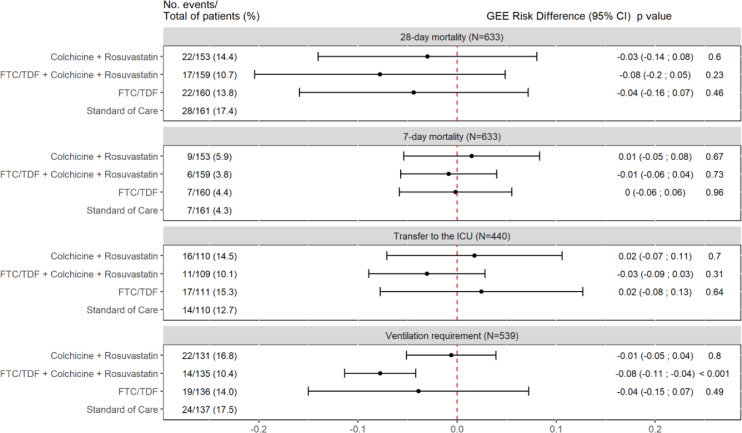
Findings: Out of 994 candidates considered between August 2020 and March 2021, 649 (65.3%) patients agreed to participate and were enrolled in this study; among them, 633 (97.5%) were included in the analysis. The mean age was 55.4 years (SD ± 12.8 years), and 428 (68%) were men; 28-day mortality was significantly lower in the FTC/TDF+COLCH+ROSUV group than in the SOC group, 10.7% (17/159) vs. 17.4% (28/161) (hazard ratio [HR] 0.53; 95% CI 0.29 to 0.96). Mortality in the FTC/TDF group was 13.8% (22/160, HR 0.68, 95% CI 0.39 to 1.20) and 14.4% in the COLCH+ROSU group (22/153) (HR 0.78, 95% CI 0.44 to 1.36). A lower need for invasive mechanical ventilation was observed in the FTC/TDF+COLCH+ROSUV group than in the SOC group (risk difference [RD] - 0.08, 95% CI 0.11 to 0.04). Three patients presented severe adverse events, one severe diarrhoea in the COLCH+ROSU and one in the FTC/TDF+COLCH+ROSU group and one general exanthema in the FTC/TDF group.
Interpretation: The combined use of FTC/TDF+COLCH+ROSU reduces the risk of 28-day mortality and the need for invasive mechanical ventilation in hospitalized patients with pulmonary compromise from COVID-19. More randomized controlled trials are needed to compare the effectiveness and cost of treatment with this combination versus other drugs that have been shown to reduce mortality from SARS-CoV-2 infection and its usefulness in patients with chronic statin use.
© 2021 The Author(s).
Conflict of interest statement
HGGD have received funding support for research (MinCiencias and Universidad Nacional de Colombia). CAM have received funding support for research (Pfizer, WHO, PAHO, Abbott and Merck), honoraria for lectures in educational events (Pfizer, Sanofi, Merck, Abbott, Biotoscana, Gilead, Roche), support for attending meeting and/or travel (Institute des Ameriques related to COVID-19), have participated on a Data Safety Monitoring Board or Advisory Board (Sanofi), and have participated in the National Committee of COVID-19 of Colombia and National COVID-19 Vaccines Committee (unpaid activities). JAC have received funding support for research (Pfizer). GB have received funding support for research (MinCiencias, Amgen Inc), and consulting fees (RTS-Baxter). All the other authors have no conflicts to declare.
Figures
Similar articles
-
Co-formulated elvitegravir, cobicistat, emtricitabine, and tenofovir disoproxil fumarate versus ritonavir-boosted atazanavir plus co-formulated emtricitabine and tenofovir disoproxil fumarate for initial treatment of HIV-1 infection: a randomised, double-blind, phase 3, non-inferiority trial.Lancet. 2012 Jun 30;379(9835):2429-2438. doi: 10.1016/S0140-6736(12)60918-0. Lancet. 2012. PMID: 22748590 Clinical Trial.
-
Co-formulated elvitegravir, cobicistat, emtricitabine, and tenofovir versus co-formulated efavirenz, emtricitabine, and tenofovir for initial treatment of HIV-1 infection: a randomised, double-blind, phase 3 trial, analysis of results after 48 weeks.Lancet. 2012 Jun 30;379(9835):2439-2448. doi: 10.1016/S0140-6736(12)60917-9. Lancet. 2012. PMID: 22748591 Clinical Trial.
-
Tenofovir Disoproxil Fumarate/Emtricitabine and Baricitinib for Patients at High Risk of Severe Coronavirus Disease 2019: The PANCOVID Randomized Clinical Trial.Clin Infect Dis. 2023 Feb 8;76(3):e116-e125. doi: 10.1093/cid/ciac628. Clin Infect Dis. 2023. PMID: 35906838 Free PMC article. Clinical Trial.
-
Daily tenofovir disoproxil fumarate/emtricitabine and hydroxychloroquine for pre-exposure prophylaxis of COVID-19: a double-blind placebo-controlled randomized trial in healthcare workers.Clin Microbiol Infect. 2023 Jan;29(1):85-93. doi: 10.1016/j.cmi.2022.07.006. Epub 2022 Aug 5. Clin Microbiol Infect. 2023. PMID: 35940567 Free PMC article. Clinical Trial.
-
Emtricitabine/tenofovir disoproxil fumarate: a review of its use in HIV-1 pre-exposure prophylaxis.Drugs. 2013 Mar;73(3):279-91. doi: 10.1007/s40265-013-0024-4. Drugs. 2013. PMID: 23444256 Review.
Cited by
-
Human Immunodeficiency Virus Status, Tenofovir Exposure, and the Risk of Poor Coronavirus Disease 19 Outcomes: Real-World Analysis From 6 United States Cohorts Before Vaccine Rollout.Clin Infect Dis. 2023 May 24;76(10):1727-1734. doi: 10.1093/cid/ciad084. Clin Infect Dis. 2023. PMID: 36861341 Free PMC article.
-
The effect of colchicine on mortality outcome and duration of hospital stay in patients with COVID-19: A meta-analysis of randomized trials.Immun Inflamm Dis. 2022 Feb;10(2):255-264. doi: 10.1002/iid3.562. Epub 2021 Dec 30. Immun Inflamm Dis. 2022. PMID: 34970856 Free PMC article.
-
NLRP3 Inflammasomes: Dual Function in Infectious Diseases.J Immunol. 2024 Aug 15;213(4):407-417. doi: 10.4049/jimmunol.2300745. J Immunol. 2024. PMID: 39102612 Free PMC article. Review.
-
Colchicine and high-intensity rosuvastatin in the treatment of non-critically ill patients hospitalised with COVID-19: a randomised clinical trial.BMJ Open. 2023 Feb 24;13(2):e067910. doi: 10.1136/bmjopen-2022-067910. BMJ Open. 2023. PMID: 36828654 Free PMC article. Clinical Trial.
-
In vitro and in silico evaluation of antiretrovirals against SARS-CoV-2: A drug repurposing approach.AIMS Microbiol. 2023 Jan 16;9(1):20-40. doi: 10.3934/microbiol.2023002. eCollection 2023. AIMS Microbiol. 2023. PMID: 36891537 Free PMC article.
References
-
- World Bank . The World Bank; 2021. Global Economic Prospects, June 2021. - DOI
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
