

Transanal Suture Mucopexy for Hemorrhoids
- PMID: 34958048
- PMCID: PMC8985695
- DOI: 10.1097/DCR.0000000000002191
Transanal Suture Mucopexy for Hemorrhoids
Abstract
Background: Core factors involved in the treatment of hemorrhoids include the engorgement of hemorrhoids, prolapse, recurrence, and pain.
Objective: The goal of this study was to assess the safety, pain, and efficacy of the transanal suture mucopexy for the treatment of hemorrhoids.
Design: This was a retrospective study over a 13-year period.
Setting: This procedure was performed, and data collected, from medical records at six centers in India.
Patients: This study includes 5634 patients who had grade II to IV symptomatic hemorrhoids. Patients suffering from thrombosed hemorrhoids, inflammatory bowel disease, anal strictures, and anorectal carcinoma were excluded.
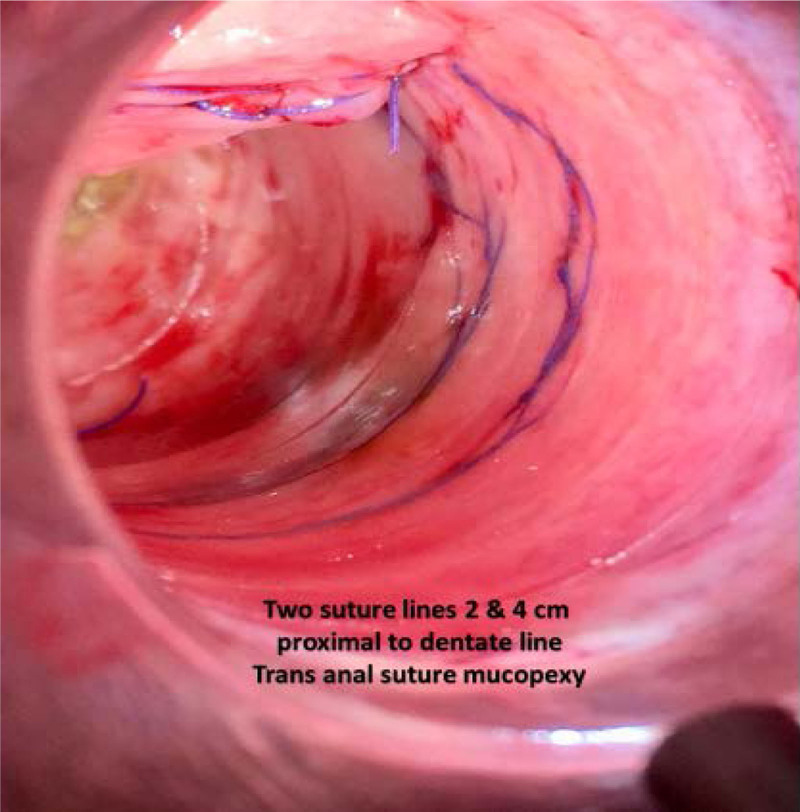
Interventions: Hemorrhoidal swelling was reduced by manual massage and a steep Trendelenburg position under saddle block. The reduced hemorrhoids were fixed to the muscles of the rectal wall using sutures. Each suture measured 0.5 to 1.0 cm in length; double-locking continuous sutures were used, along the complete circumference of the rectum, at 2 and 4 cm proximal to the dentate line.
Main outcome measures: Pain assessed using the visual analog scale and hemorrhoid recurrence served as outcome measures.
Results: The transanal suture mucopexy procedure was performed for 5634 patients with symptomatic hemorrhoids. A dull pain compatible with a visual analog score of 2 to 3 was reported in 126 (2.2%) patients; in the remaining 5508 (97.8%) patients, the visual analog score was 1 to 2. Effective treatment without complications occurred for 5541 patients (98.65%). A recurrence rate of 1.3% was recorded in 5634 cases with a mean follow-up of 7 ± 6 years.
Limitations: Utilization of a self-illuminating proctoscope or Brinckerhoff or anal speculum is essential.
Conclusion: Transanal suture mucopexy, designed with 2 suture rows, is a safe procedure with a short learning curve. It is associated with minimal pain, low recurrence rate, and fewer complications. See Video Abstract at http://links.lww.com/DCR/B841.
Mucopexia transanal con sutura para enfermedad hemorroidal: ANTECEDENTES:Los factores centrales involucrados en el tratamiento de la enfermedad hemorroidal incluyen congestión de hemorroides, prolapso, recurrencia y dolor.OBJETIVO:Evaluar la seguridad, el dolor y la eficacia de la mucopexia transanal con sutura para el tratamiento de la enfermedad hemorroidal.DISEÑO:Estudio retrospectivo durante un período de 13 años.ESCENARIO:Este procedimiento se realizó y se recopilaron datos de expedientes médicos en seis centros en India.PACIENTES:Este estudio incluye 5634 pacientes con enfermedad hemorroidal sintomática grado II a IV. Se excluyeron pacientes que padecían hemorroides trombosadas, enfermedad inflamatoria intestinal, estenosis anales y carcinoma anorrectal.INTERVENCIONES:La inflamación hemorroidal se redujo mediante masaje manual y posición Trendelenburg profundo bajo bloqueo caudal. Las hemorroides reducidas se fijaron a los músculos de la pared rectal mediante suturas. Cada sutura midió 0.5 a 1.0 cm de longitud, se utilizaron suturas en surgete continuo de doble anclado, a lo largo de la circunferencia completa del recto, a dos y cuatro cm proximales a la línea dentada.PRINCIPALES MEDIDAS DE RESULTADO:El dolor se evaluó mediante la escala de puntuación analógica visual y se evaluó la presencia de recurrencia.RESULTADOS:El procedimiento de mucopexia transanal con sutura se realizó en 5634 pacientes con hemorroides sintomáticas. Se informó un dolor sordo compatible con una puntuación analógica visual de 2-3 en 126 (2.2%) pacientes; en los 5508 (97.8%) pacientes restantes, la puntuación analógica visual fue de 1-2. La mayoría (5541 pacientes [98.65%]) tuvo un tratamiento eficaz sin complicaciones. Se registró una tasa de recurrencia del 1.3% en 5634 casos con un seguimiento medio de 7 ± 6 años.LIMITACIONES:La utilización de un proctoscopio autoiluminado o de Brinckerhoff o espéculo anal es esencial.CONCLUSIÓN:La mucopexia transanal con sutura es un procedimiento seguro diseñado con dos filas de suturas asociadas con dolor mínimo y baja tasa de recurrencia con menos complicaciones. Tiene una curva de aprendizaje corta. Consulte Video Resumen en http://links.lww.com/DCR/B841. (Traducción-Dr. Jorge Silva Velazco).
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Society of Colon and Rectal Surgeons.
Figures





References
-
- Loder PB, Kamm MA, Nicholls RJ, Phillips RK. Haemorrhoids: pathology, pathophysiology and aetiology. Br J Surg. 1994;81:946–954. - PubMed
-
- Parks AG. De haemorrhois; a study in surgical history. Guys Hosp Rep. 1955;104:135–156. - PubMed
-
- Tewari M, Shukla HS. Sushrusha the father of Indian surgery. Indian J Surg. 2005;67:229–230.
-
- Milligan ETC, Morgan CN, Officer R. Surgical anatomy of the anal canal, and the operative treatment of haemorrhoids. Lancet. 1937;230:1119–1124.
-
- Thomson WH. The nature of haemorrhoids. Br J Surg. 1975;62:542–552. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
