

Safety of MRI in patients with retained cardiac leads
- PMID: 34958685
- PMCID: PMC8919805
- DOI: 10.1002/mrm.29116
Safety of MRI in patients with retained cardiac leads
Abstract
Purpose: To evaluate the safety of MRI in patients with fragmented retained leads (FRLs) through numerical simulation and phantom experiments.
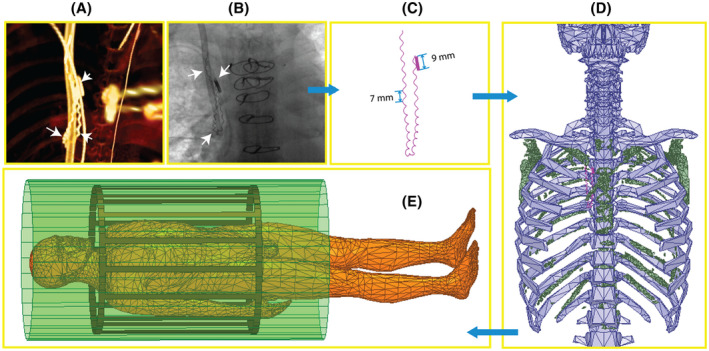
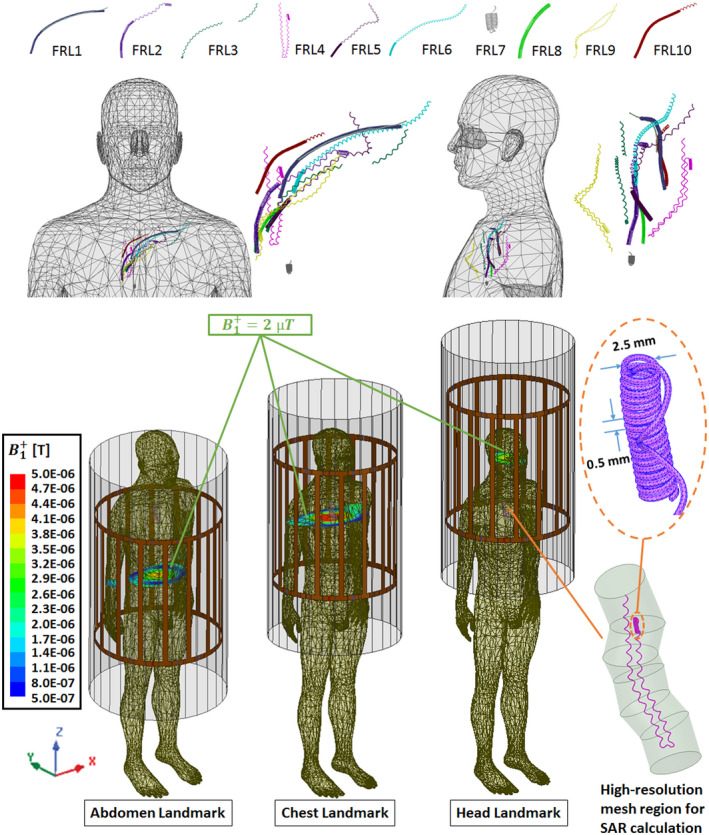
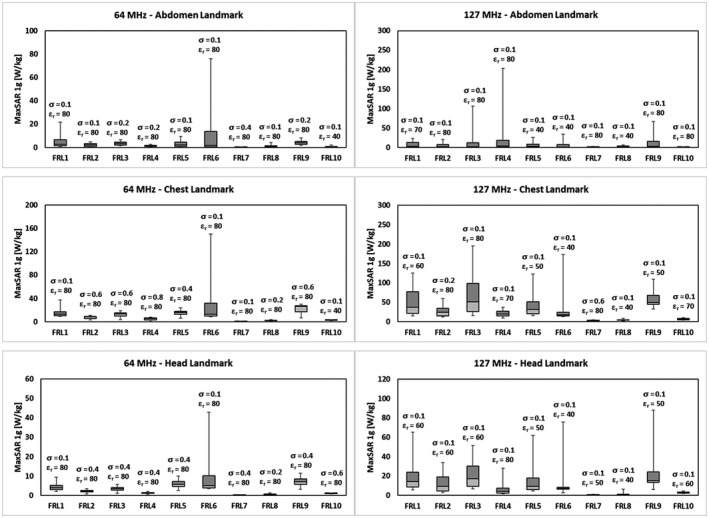
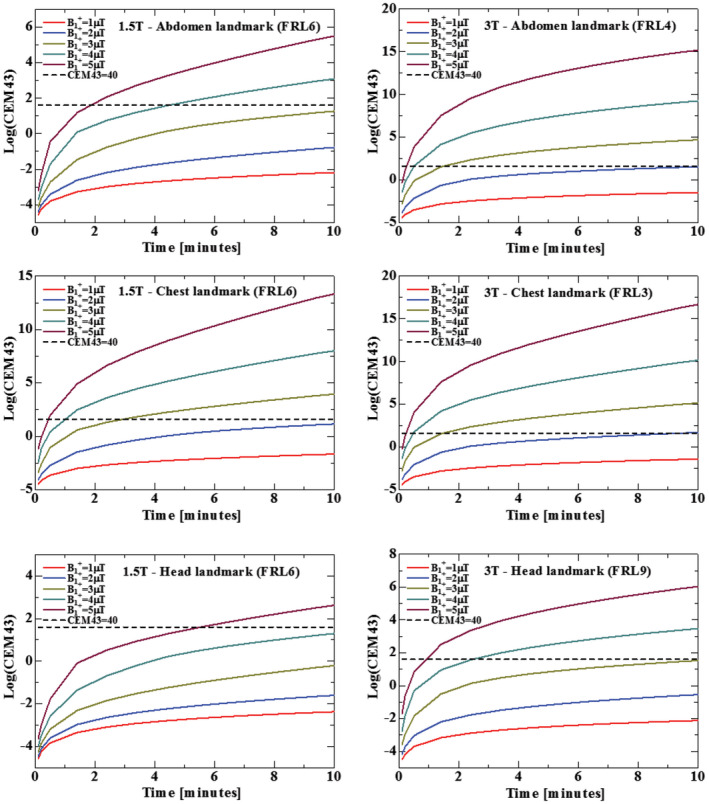
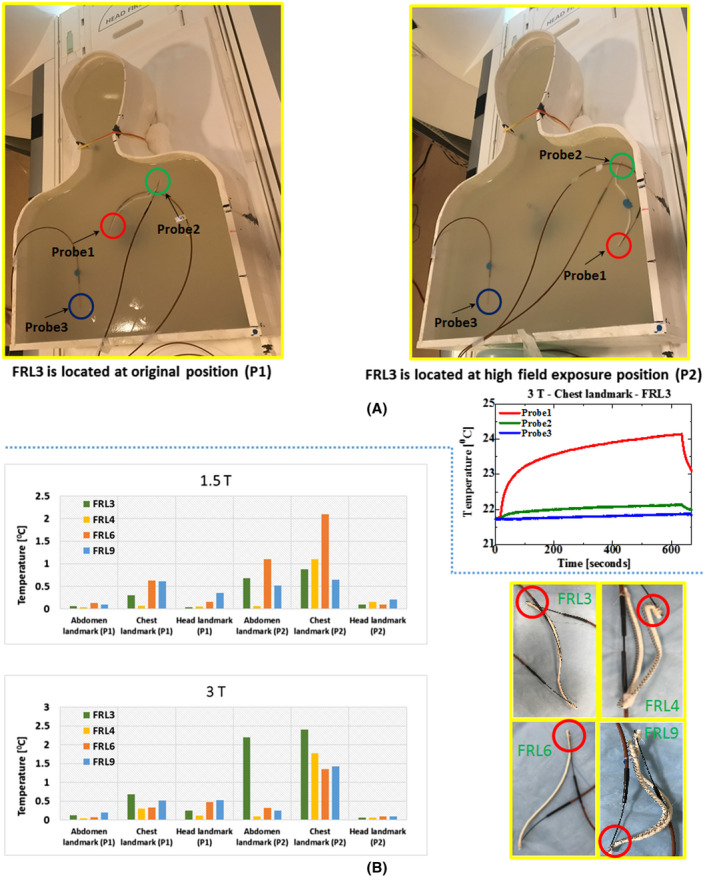
Methods: Electromagnetic and thermal simulations were performed to determine the worst-case RF heating of 10 patient-derived FRL models during MRI at 1.5 T and 3 T and at imaging landmarks corresponding to head, chest, and abdomen. RF heating measurements were performed in phantoms implanted with reconstructed FRL models that produced highest heating in numerical simulations. The potential for unintended tissue stimulation was assessed through a conservative estimation of the electric field induced in the tissue due to gradient-induced voltages developed along the length of FRLs.
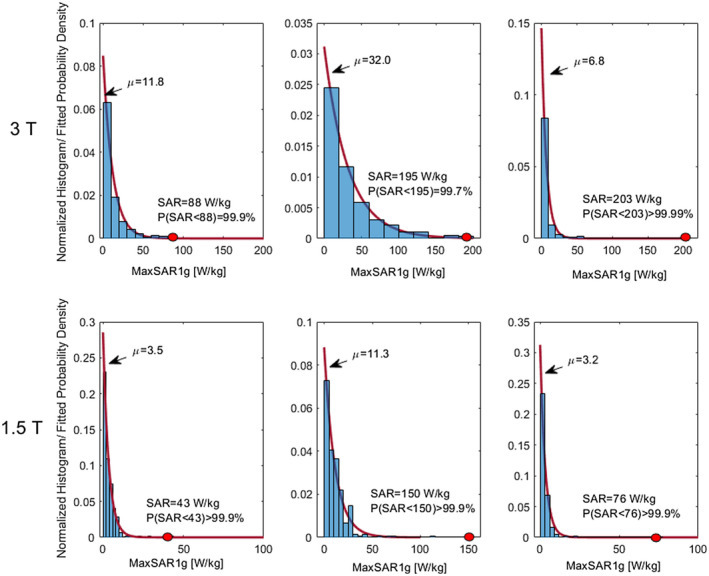
Results: In simulations under conservative approach, RF exposure at B1+ ≤ 2 µT generated cumulative equivalent minutes (CEM)43 < 40 at all imaging landmarks at both 1.5 T and 3 T, indicating no thermal damage for acquisition times (TAs) < 10 min. In experiments, the maximum temperature rise when FRLs were positioned at the location of maximum electric field exposure was measured to be 2.4°C at 3 T and 2.1°C at 1.5 T. Electric fields induced in the tissue due to gradient-induced voltages remained below the threshold for cardiac tissue stimulation in all cases.
Conclusions: Simulation and experimental results indicate that patients with FRLs can be scanned safely at both 1.5 T and 3 T with most clinical pulse sequences.
Keywords: RF heating; SAR; cardiovascular implantable electronic devices; finite element methods; fragmented retained leads; safety.
© 2021 The Authors. Magnetic Resonance in Medicine published by Wiley Periodicals LLC on behalf of International Society for Magnetic Resonance in Medicine.
Figures
References
-
- Greenspon AJ, Patel JD, Lau E, et al. Trends in permanent pacemaker implantation in the United States from 1993 to 2009: increasing complexity of patients and procedures. J Am Coll Cardiol. 2012;60:1540‐1545. - PubMed
-
- Sommer T, Naehle CP, Yang A, et al. Strategy for safe performance of extrathoracic magnetic resonance imaging at 1.5 Tesla in the presence of cardiac pacemakers in non–pacemaker‐dependent patients a prospective study with 115 examinations. Circulation. 2006;114:1285‐1292. - PubMed
-
- Kalin R, Stanton MS. Current clinical issues for MRI scanning of pacemaker and defibrillator patients. Pacing Clin Electrophysiol. 2005;28:326‐328. - PubMed
-
- Naehle CP, Zeijlemaker V, Thomas D, et al. Evaluation of cumulative effects of MR imaging on pacemaker systems at 1.5 Tesla. Pacing Clin Electrophysiol. 2009;32:1526‐1535. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
