

Past and Future of Phage Therapy and Phage-Derived Proteins in Patients with Bone and Joint Infection
- PMID: 34960683
- PMCID: PMC8708067
- DOI: 10.3390/v13122414
Past and Future of Phage Therapy and Phage-Derived Proteins in Patients with Bone and Joint Infection
Abstract
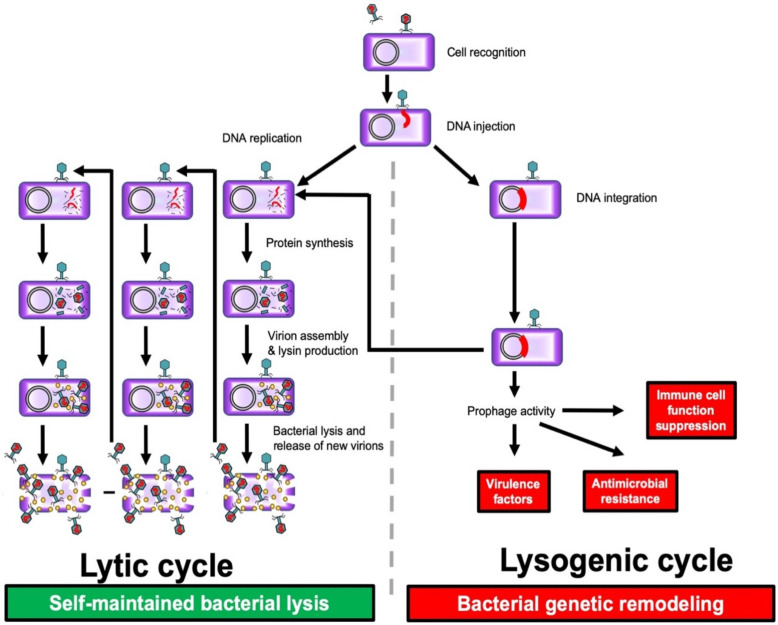
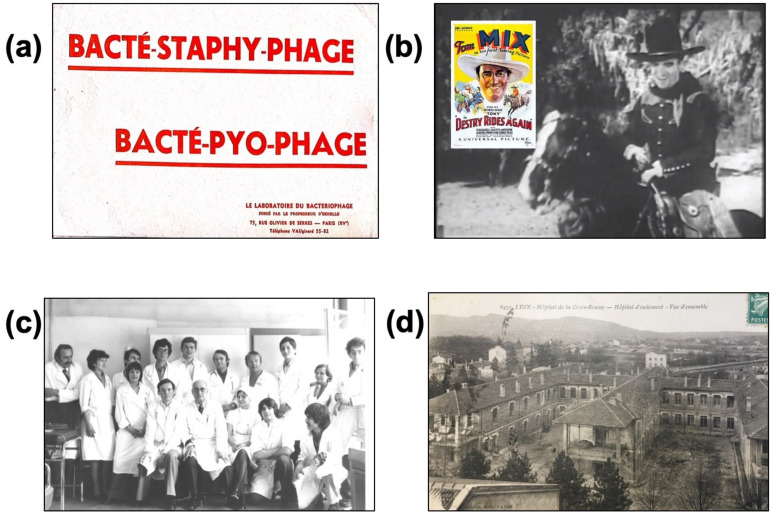
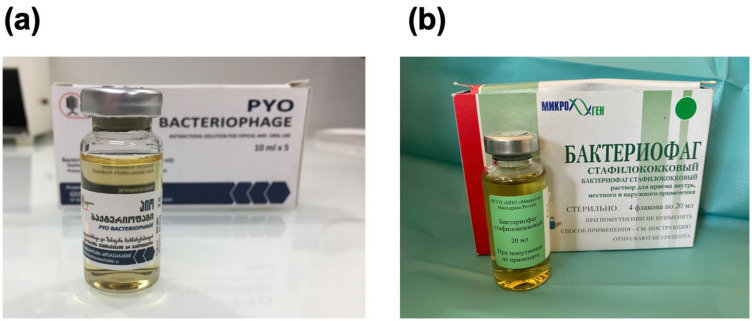
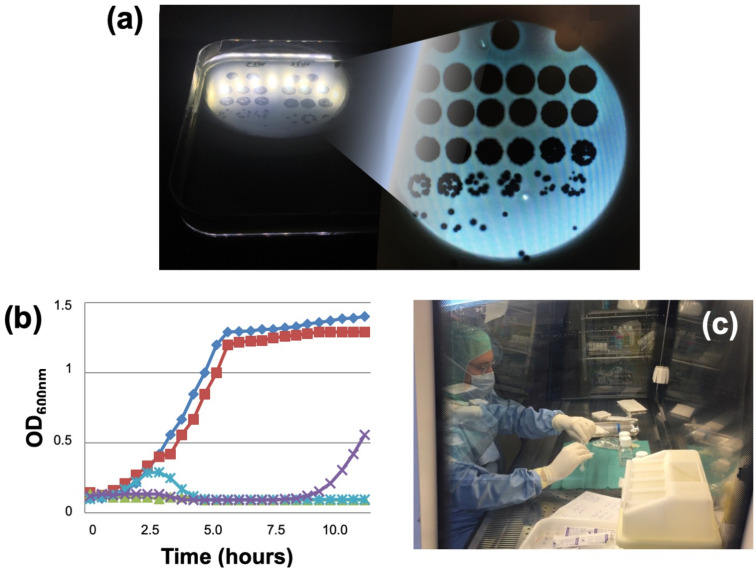
Phage-derived therapies comprise phage therapy and the use of phage-derived proteins as anti-bacterial therapy. Bacteriophages are natural viruses that target specific bacteria. They were proposed to be used to treat bacterial infections in the 1920s, before the discovery and widespread over-commercialized use of antibiotics. Phage therapy was totally abandoned in Western countries, whereas it is still used in Poland, Georgia and Russia. We review here the history of phage therapy by focusing on bone and joint infection, and on the development of phage therapy in France in this indication. We discuss the rationale of its use in bacterial infection and show the feasibility of phage therapy in the 2020s, based on several patients with complex bone and joint infection who recently received phages as compassionate therapy. Although the status of phage therapy remains to be clarified by health care authorities, obtaining pharmaceutical-grade therapeutic phages (i.e., following good manufacturing practice guidelines or being "GMP-like") targeting bacterial species of concern is essential. Moreover, multidisciplinary clinical expertise has to determine what could be the relevant indications to perform clinical trials. Finally "phage therapy 2.0" has to integrate the following steps: (i) follow the status of phage therapy, that is not settled and defined; (ii) develop in each country a close relationship with the national health care authority; (iii) develop industrial-academic partnerships; (iv) create academic reference centers; (v) identify relevant clinical indications; (vi) use GMP/GMP-like phages with guaranteed quality bioproduction; (vii) start as salvage therapy; (vii) combine with antibiotics and adequate surgery; and (viii) perform clinical trials, to finally (ix) demonstrate in which clinical settings phage therapy provides benefit. Phage-derived proteins such as peptidoglycan hydrolases, polysaccharide depolymerases or lysins are enzymes that also have anti-biofilm activity. In contrast to phages, their development has to follow the classical process of medicinal products. Phage therapy and phage-derived products also have a huge potential to treat biofilm-associated bacterial diseases, and this is of crucial importance in the worldwide spread of antimicrobial resistance.
Keywords: ANSM drug-safety agency; bacteriophages; bone and joint infection; compassionate use; lysin; osteoarticular infection; osteomyelitis; phage therapy; phage-derived enzyme; prosthetic joint infection.
Conflict of interest statement
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. TF received a speaker honorarium from ContraFect (IDWeek 2019, Washington, USA). Hospices Civils de Lyon received a research grant from French authorities in 2014 for the PHOSA project that was finished in 2017.
Figures
References
-
- Ferry T., Kolenda C., Gustave C.-A., Lustig S., Josse J., Batailler C., Pirot F., Leboucher G., Laurent F. Phagothérapie pour les patients présentant une infection osteoarticulaire: Historique, fondements, faisabilité et perspectives en France. Virologie. 2020;24:49–56. doi: 10.1684/vir.2020.0808. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
