

Efficacy of a technology-based client-centred training system in neurological rehabilitation: a randomised controlled trial
- PMID: 34961531
- PMCID: PMC8712106
- DOI: 10.1186/s12984-021-00977-2
Efficacy of a technology-based client-centred training system in neurological rehabilitation: a randomised controlled trial
Abstract
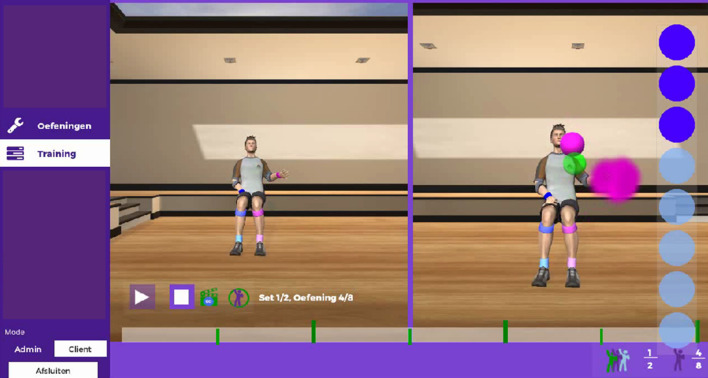
Background: A client-centred task-oriented approach has advantages towards motivation and adherence to therapy in neurorehabilitation, but it is costly to integrate in practice. An intelligent Activity-based Client-centred Training (i-ACT), a low-cost Kinect-based system, was developed which integrates a client-centred and task-oriented approach. The objectives were (1) to investigate the effect of additional i-ACT training on functioning. And (2) to assess whether training with i-ACT resulted in more goal oriented training.
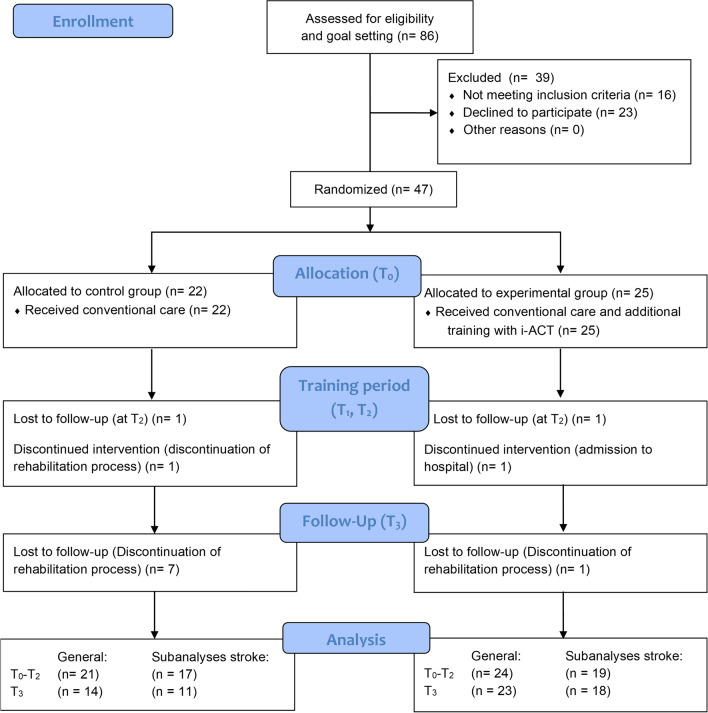
Methods: A single-blind randomised controlled trial was performed in 4 Belgian rehabilitation centres with persons with central nervous system deficits. Participants were randomly allocated through an independent website-based code generator using blocked randomisation (n = 4) to an intervention or control group. The intervention group received conventional care and additional training with i-ACT for 3 × 45 min/week during 6 weeks. The control group received solely conventional care. Functional ability and performance, quality of life (QoL), fatigue, trunk movement, and shoulder active range of motion (AROM) were assessed at baseline, after 3 weeks and 6 weeks of training, and 6 weeks after cessation of training. Data were analysed using non-parametric within and between group analysis.
Results: 47 persons were randomised and 45 analysed. Both intervention (n = 25) and control (n = 22) group improved over time on functional ability and performance as measured by the Wolf Motor Function Test, Manual Ability Measure-36, and Canadian Occupational Performance Measure, but no major differences were found between the groups on these primary outcome measures. Regarding QoL, fatigue, trunk movement, and shoulder AROM, no significant between group differences were found. High adherence for i-ACT training was found (i.e. 97.92%) and no adverse events, linked to i-ACT, were reported. In the intervention group the amount of trained personal goals (88%) was much higher than in the control group (46%).
Conclusions: Although additional use of i-ACT did not have a statistically significant added value regarding functional outcome over conventional therapy, additional i-ACT training provides more individualised client-centred therapy, and adherence towards i-ACT training is high. A higher intensity of i-ACT training may increase therapy effects, and should be investigated in future research.
Trial registration: ClinicalTrials.gov Identifier NCT02982811. Registered 29 November 2016.
Keywords: Client-centred; Efficacy; Rehabilitation; Task-oriented; Technology.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Motivation, Usability, and Credibility of an Intelligent Activity-Based Client-Centred Training System to Improve Functional Performance in Neurological Rehabilitation: An Exploratory Cohort Study.Int J Environ Res Public Health. 2021 Jul 18;18(14):7641. doi: 10.3390/ijerph18147641. Int J Environ Res Public Health. 2021. PMID: 34300092 Free PMC article.
-
Developing an intelligent activity-based client-centred training system with a user-centred approach.Technol Health Care. 2020;28(4):355-368. doi: 10.3233/THC-191854. Technol Health Care. 2020. PMID: 31796713
-
A cluster randomised controlled trial on the efficacy of client-centred occupational therapy in multiple sclerosis: good process, poor outcome.Disabil Rehabil. 2013 Sep;35(19):1636-46. doi: 10.3109/09638288.2012.748845. Epub 2013 Jan 24. Disabil Rehabil. 2013. PMID: 23343363 Clinical Trial.
-
Effectiveness of robot-assisted training added to conventional rehabilitation in patients with humeral fracture early after surgical treatment: protocol of a randomised, controlled, multicentre trial.Trials. 2017 Dec 6;18(1):589. doi: 10.1186/s13063-017-2274-z. Trials. 2017. PMID: 29212528 Free PMC article. Clinical Trial.
-
Erratum.Mult Scler. 2016 Oct;22(12):NP9-NP11. doi: 10.1177/1352458515585718. Epub 2015 Jun 3. Mult Scler. 2016. PMID: 26041800
References
-
- Brokaw EB, Eckel E, Brewer BR. Usability evaluation of a kinematics focused Kinect therapy program for individuals with stroke. THC. 2015;23(2):143–151. - PubMed
-
- Saposnik G, Levin M, Outcome Research Canada Working G Virtual reality in stroke rehabilitation: a meta-analysis and implications for clinicians. Stroke. 2011;42(5):1380–1386. - PubMed
-
- Sin H, Lee G. Additional virtual reality training using Xbox Kinect in stroke survivors with hemiplegia. Am J Phys Med Rehabil. 2013;92(10):871–880. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
