

doi: 10.1016/j.biopsych.2021.11.004.
"I Am Not I": The Neuroscience of Dissociative Identity Disorder
Affiliations
- PMID: 34961597
- PMCID: PMC9045405
- DOI: 10.1016/j.biopsych.2021.11.004
Item in Clipboard
"I Am Not I": The Neuroscience of Dissociative Identity Disorder
Biol Psychiatry.
.
No abstract available
Figures
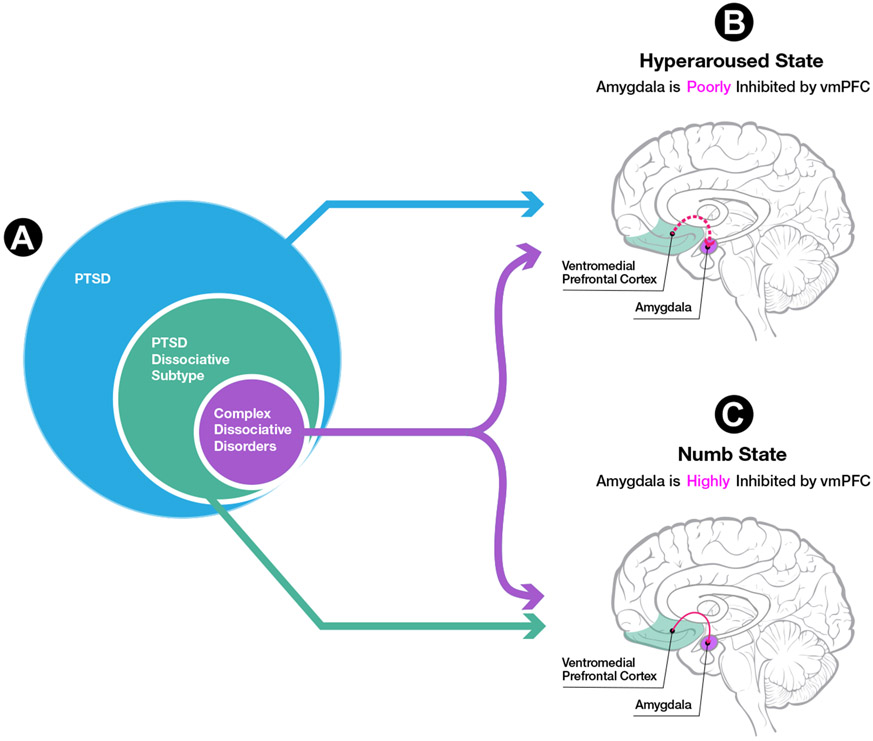
(A) Conventional posttraumatic stress disorder (PTSD) is characterized by a dominance of hyperarousal symptoms. In contrast, 15% to 30% of individuals with PTSD have the dissociative subtype characterized by symptoms of depersonalization and derealization—that is, feeling numb and detached from their sense of self, body, and environment. Within the PTSD dissociative subtype group, approximately half of individuals have more extensive dissociative symptoms, including individuals who meet criteria for dissociative identity disorder (DID). In neuroimaging studies of DID, researchers have asked subjects to shift between two prototypical self-states: one that feels hyperaroused, emotionally flooded, and like the traumatic event happened to them personally; and one that feels numb and detached, as if the traumatic event did not happen to them personally. (B) Typical findings for conventional PTSD during symptom provocation paradigms, including increased limbic activity (e.g., amygdala) and decreased cortical emotion regulation–related activity (e.g., ventromedial prefrontal cortex [vmPFC]). Together these findings demonstrate, on average, undermodulation of emotion and arousal in conventional PTSD. Individuals with DID also exhibit this pattern in symptom provocation paradigms when they are in a hyperaroused self-state, as described above. (C) In contrast, panel (C) illustrates typical findings for the dissociative subtype of PTSD during symptom provocation paradigms, including decreased limbic activity (e.g., amygdala) and increased cortical emotion regulation-related activity (e.g., vmPFC). These findings support, on average, a pattern of emotion/arousal overmodulation in the dissociative subtype of PTSD. Individuals with DID also exhibit this overmodulation pattern in symptom provocation paradigms when they are in a numb self-state, as described above.
References
-
- Ellenberger HF (1970). The Discovery of the Unconscious: The History and Evolution of Dynamic Psychiatry, vol. 1. New York: Basic Books.
-
- Freud S (1985): Letter from Freud to Fliess, September 21, 1897. In: Masson JM, editor. The Complete Letters of Sigmund Freud to Wilhelm Fliess, 1887-1904. Cambridge, MA, and London, England: The Belknap Press of Harvard University Press, 264–267.
-
- Yehuda R, Southwick S, Giller EL, Ma X, Mason JW (1992): Urinary catecholamine excretion and severity of PTSD symptoms in Vietnam combat veterans. J Nerv Ment Dis 180:321–325. - PubMed
-
- Rauch SL, van der Kolk BA, Fisler RE, Alpert NM, Orr SP, Savage CR, et al. (1996): A symptom provocation study of posttraumatic stress disorder using positron emission tomography and script-driven imagery. Arch Gen Psychiatry 53:380–387. - PubMed
-
- Lanius RA, Boyd JE, McKinnon MC, Nicholson AA, Frewen P, Vermetten E, et al. (2018): A review of the neurobiological basis of trauma-related dissociation and its relation to cannabinoid-and opioid-mediated stress response: A transdiagnostic, translational approach. Curr Psychiatry Rep 20:118–132. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
