

Computationally prioritized drugs inhibit SARS-CoV-2 infection and syncytia formation
- PMID: 34962256
- PMCID: PMC8769897
- DOI: 10.1093/bib/bbab507
Computationally prioritized drugs inhibit SARS-CoV-2 infection and syncytia formation
Abstract
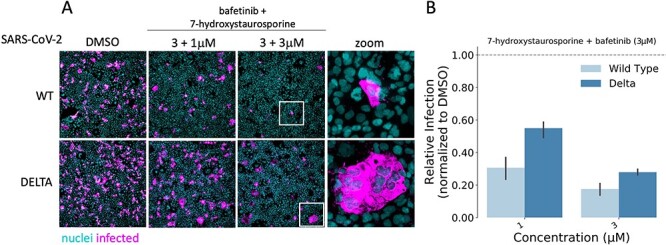
The pharmacological arsenal against the COVID-19 pandemic is largely based on generic anti-inflammatory strategies or poorly scalable solutions. Moreover, as the ongoing vaccination campaign is rolling slower than wished, affordable and effective therapeutics are needed. To this end, there is increasing attention toward computational methods for drug repositioning and de novo drug design. Here, multiple data-driven computational approaches are systematically integrated to perform a virtual screening and prioritize candidate drugs for the treatment of COVID-19. From the list of prioritized drugs, a subset of representative candidates to test in human cells is selected. Two compounds, 7-hydroxystaurosporine and bafetinib, show synergistic antiviral effects in vitro and strongly inhibit viral-induced syncytia formation. Moreover, since existing drug repositioning methods provide limited usable information for de novo drug design, the relevant chemical substructures of the identified drugs are extracted to provide a chemical vocabulary that may help to design new effective drugs.
Keywords: 7-hydroxystaurosporine; COVID-19; SARS-CoV-2; bafetinib; delta variant; drug design; drug repositioning; kinase inhibitors; syncytia; virtual screening.
© The Author(s) 2021. Published by Oxford University Press.
Figures








References
-
- Thanh Le T, Andreadakis Z, Kumar A, et al. The COVID-19 vaccine development landscape. Nat Rev Drug Discov 2020;19:305–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
