

The giant steps in surgical downsizing toward a personalized treatment of vulvar cancer
- PMID: 34962334
- PMCID: PMC9302990
- DOI: 10.1111/jog.15103
The giant steps in surgical downsizing toward a personalized treatment of vulvar cancer
Abstract
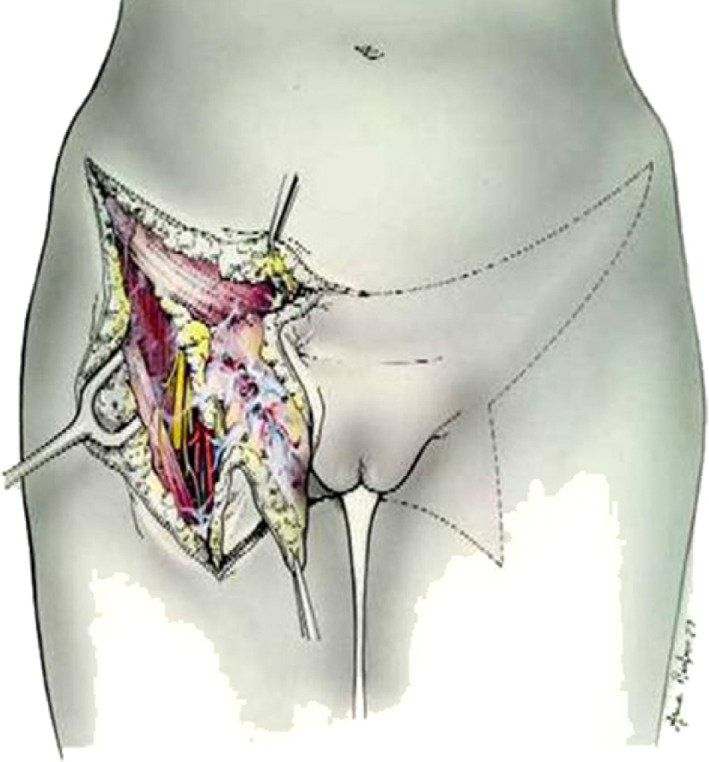
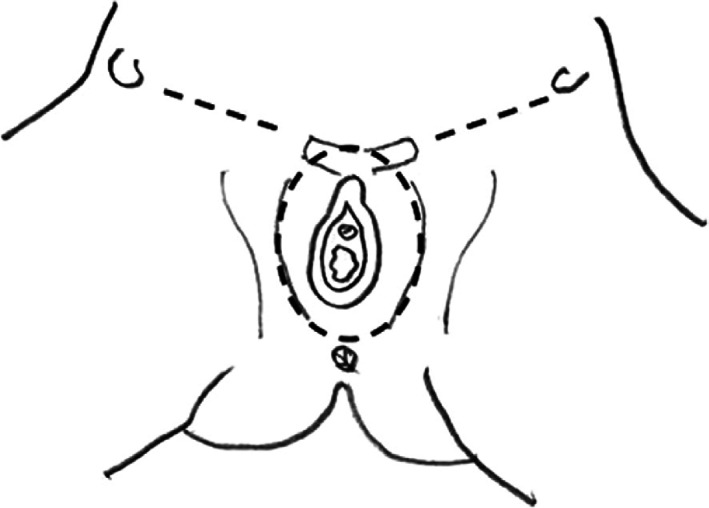
The present article aims to highlight the importance of changes of personalized surgical treatment for vulvar cancer. Current international literature regarding surgical treatment of vulvar cancer was evaluated. This included several studies and systematic reviews. Radical surgery approach, such as en bloc resection, was the first therapeutic option and the standard care for many years, even if burdened with a high complication rate and frequently disfiguring. Taussing and Way introduced radical vulvectomy approach with en bloc bilateral inguinal-femoral lymphadenectomy; modified radical vulvectomy was developed, with a wide radical excision of the primary tumor. The role of inguinofemoral lymphadenectomy (mono or bilateral) changed in the years too, particularly with the advent of SLN biopsy as minimally invasive surgical approach for lymph node staging, in patients with unifocal cancer <4 cm, without suspicious groin nodes. More personalized and conservative surgical approach, consisting of wide local or wide radical excisions, is necessary to reduce complications as lymphedema or sexual disfunction. The optimal surgical management of vulvar cancer needs to consider dimensions, staging, depth of invasion, presence of carcinoma at the surgical margins of resection and grading, with the goal of making the treatment as individualized as possible.
Keywords: Taylor therapy; inguinofemoral lymphadenectomy; radical vulvectomy; sentinel lymph node biopsy; vulvar cancer.
© 2021 The Authors. Journal of Obstetrics and Gynaecology Research published by John Wiley & Sons Australia, Ltd on behalf of Japan Society of Obstetrics and Gynecology.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Vulvar cancer – cancer stat facts. 2018. [cited Aug 29]. Available from: https://seer.cancer.gov/statfacts/html/vulva.html
-
- Bayne L, Butler J, Colombo N, Geissler J, Green J, Kesic VI, et al. Gynaecological cancers in Europe: facts and figures 2015. ASACO website [cited 2019 May 30].
-
- Greer BE, Koh WJ. New NCCN guidelines for vulvar cancer. J Natl Compr Canc Netw. 2016;14:656–8. - PubMed
-
- Hacker NF, Eifel PJ, van der Velden J. Cancer of the vulva. Int J Gynaecol Obstet. 2012;119(2):S90–6. - PubMed
-
- Del Pino M, Rodriguez‐Carunchio L, Ordi J. Pathways of vulvar intraepithelial neoplasia and squamous cell carcinoma. Histopathology. 2013;62(1):161–75. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
