

B Cell Numbers Predict Humoral and Cellular Response Upon SARS-CoV-2 Vaccination Among Patients Treated With Rituximab
- PMID: 34962360
- PMCID: PMC9011692
- DOI: 10.1002/art.42060
B Cell Numbers Predict Humoral and Cellular Response Upon SARS-CoV-2 Vaccination Among Patients Treated With Rituximab
Abstract
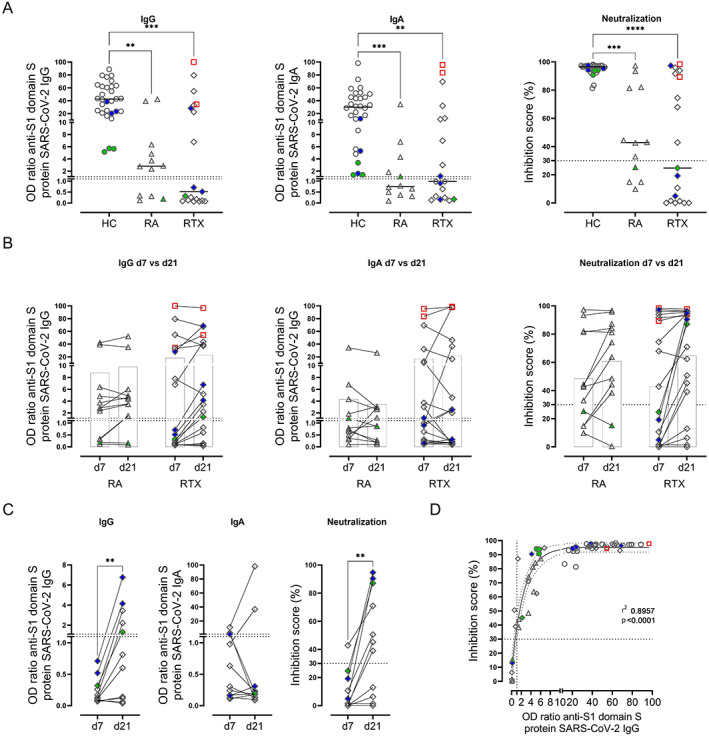
Objective: Patients with autoimmune inflammatory rheumatic diseases receiving rituximab (RTX) therapy are at higher risk of poor COVID-19 outcomes and show substantially impaired humoral immune response to anti-SARS-CoV-2 vaccine. However, the complex relationship between antigen-specific B cells and T cells and the level of B cell repopulation necessary to achieve anti-vaccine responses remain largely unknown.
Methods: Antibody responses to SARS-CoV-2 vaccines and induction of antigen-specific B and CD4/CD8 T cell subsets were studied in 19 patients with rheumatoid arthritis (RA) or antineutrophil cytoplasmic antibody-associated vasculitis receiving RTX, 12 patients with RA receiving other therapies, and 30 healthy controls after SARS-CoV-2 vaccination with either messenger RNA or vector-based vaccines.
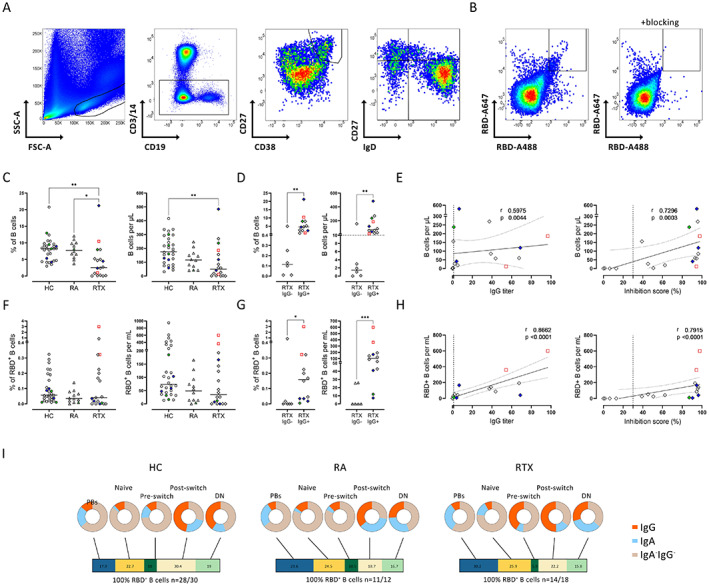
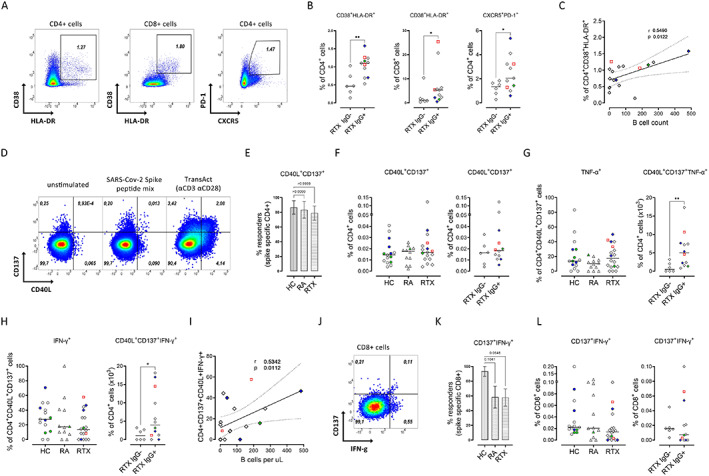
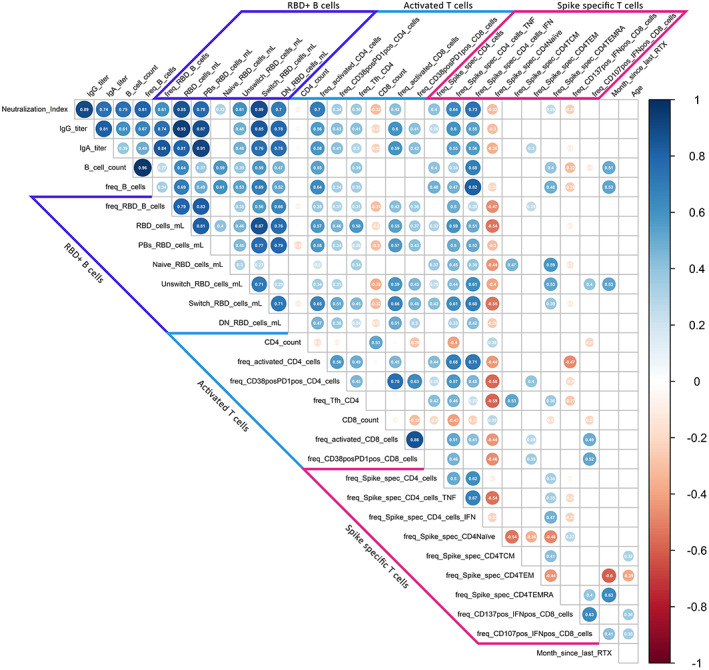
Results: A minimum of 10 B cells per microliter (0.4% of lymphocytes) in the peripheral circulation appeared to be required for RTX-treated patients to mount seroconversion to anti-S1 IgG upon SARS-CoV-2 vaccination. RTX-treated patients who lacked IgG seroconversion showed reduced receptor-binding domain-positive B cells (P = 0.0005), a lower frequency of Tfh-like cells (P = 0.0481), as well as fewer activated CD4 (P = 0.0036) and CD8 T cells (P = 0.0308) compared to RTX-treated patients who achieved IgG seroconversion. Functionally relevant B cell depletion resulted in impaired interferon-γ secretion by spike-specific CD4 T cells (P = 0.0112, r = 0.5342). In contrast, antigen-specific CD8 T cells were reduced in both RA patients and RTX-treated patients, independently of IgG formation.
Conclusion: In RTX-treated patients, a minimum of 10 B cells per microliter in the peripheral circulation is a candidate biomarker for a high likelihood of an appropriate cellular and humoral response after SARS-CoV-2 vaccination. Mechanistically, the data emphasize the crucial role of costimulatory B cell functions for the proper induction of CD4 responses propagating vaccine-specific B cell and plasma cell differentiation.
© 2021 The Authors. Arthritis & Rheumatology published by Wiley Periodicals LLC on behalf of American College of Rheumatology.
Figures

Comment in
-
B cells: deplete, repopulate, vaccinate.Nat Rev Rheumatol. 2022 Mar;18(3):126. doi: 10.1038/s41584-022-00754-y. Nat Rev Rheumatol. 2022. PMID: 35110747 Free PMC article.
References
-
- Furer V, Rondaan C, Heijstek M, van Assen S, Bijl M, Agmon‐Levin N, et al. Incidence and prevalence of vaccine preventable infections in adult patients with autoimmune inflammatory rheumatic diseases (AIIRD): a systemic literature review informing the 2019 update of the EULAR recommendations for vaccination in adult patients with AIIRD. RMD Open 2019;5:e001041. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
