

Invasive Right Ventricular Pressure-Volume Analysis: Basic Principles, Clinical Applications, and Practical Recommendations
- PMID: 34963308
- PMCID: PMC8766922
- DOI: 10.1161/CIRCHEARTFAILURE.121.009101
Invasive Right Ventricular Pressure-Volume Analysis: Basic Principles, Clinical Applications, and Practical Recommendations
Abstract
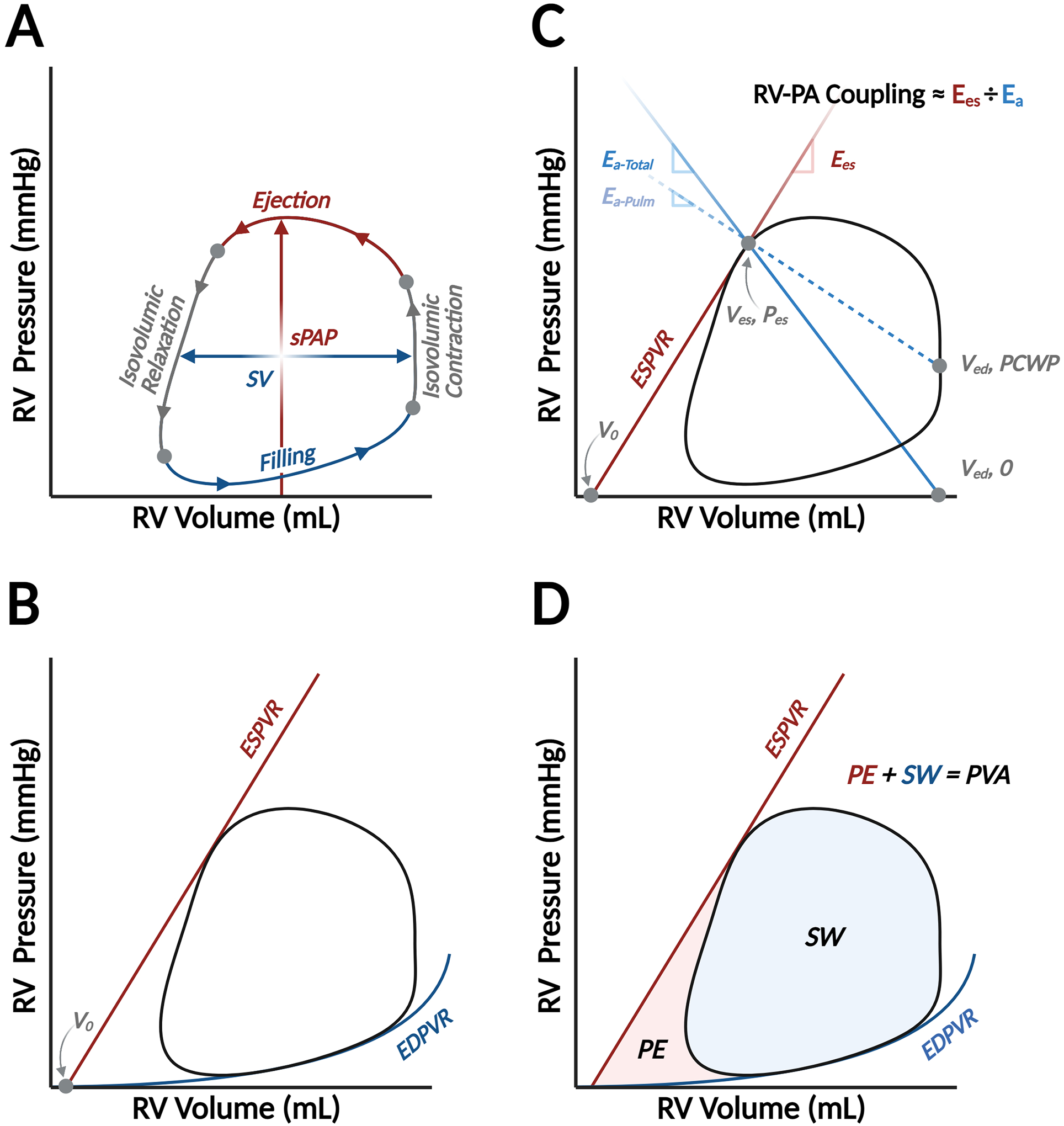
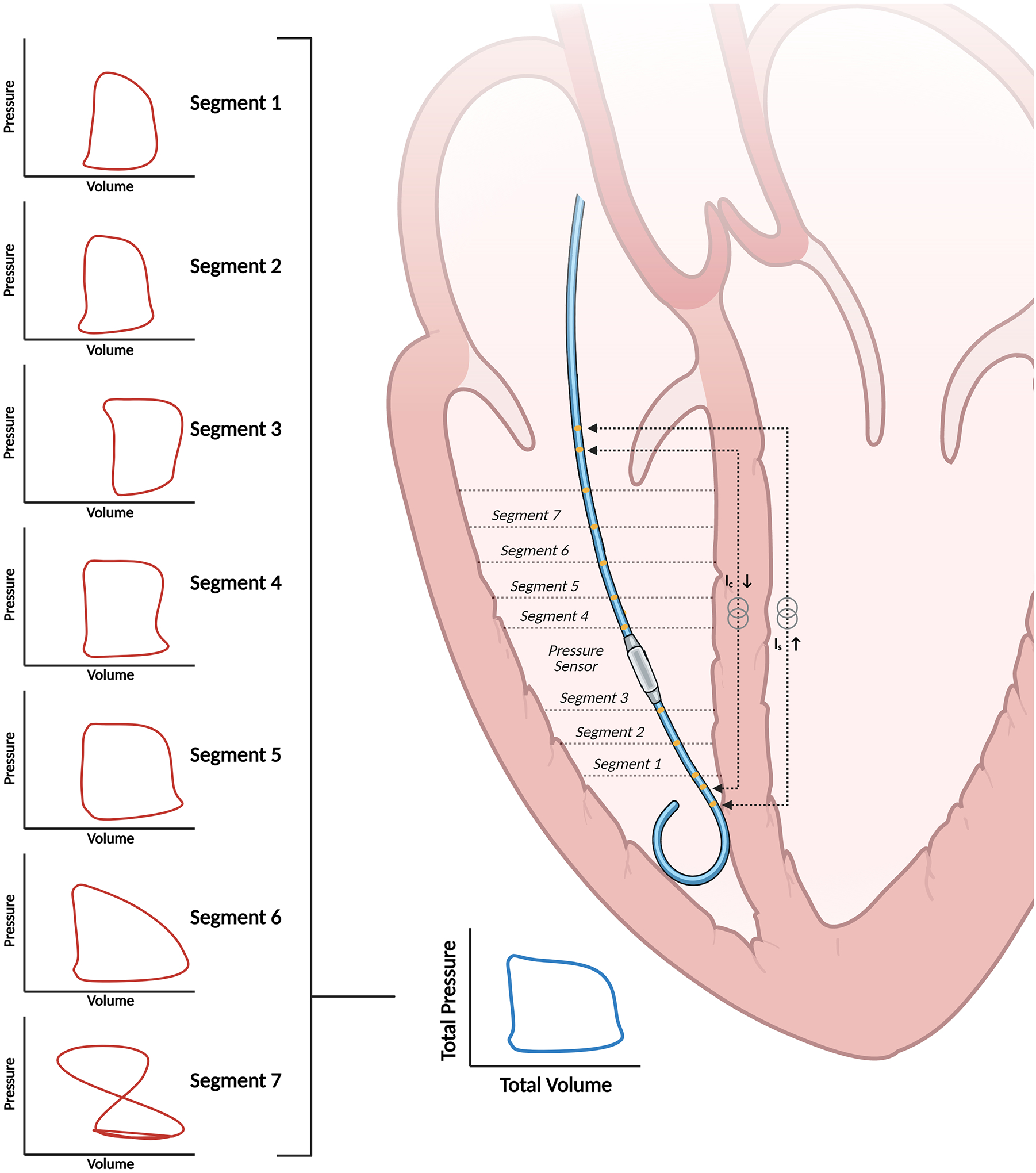
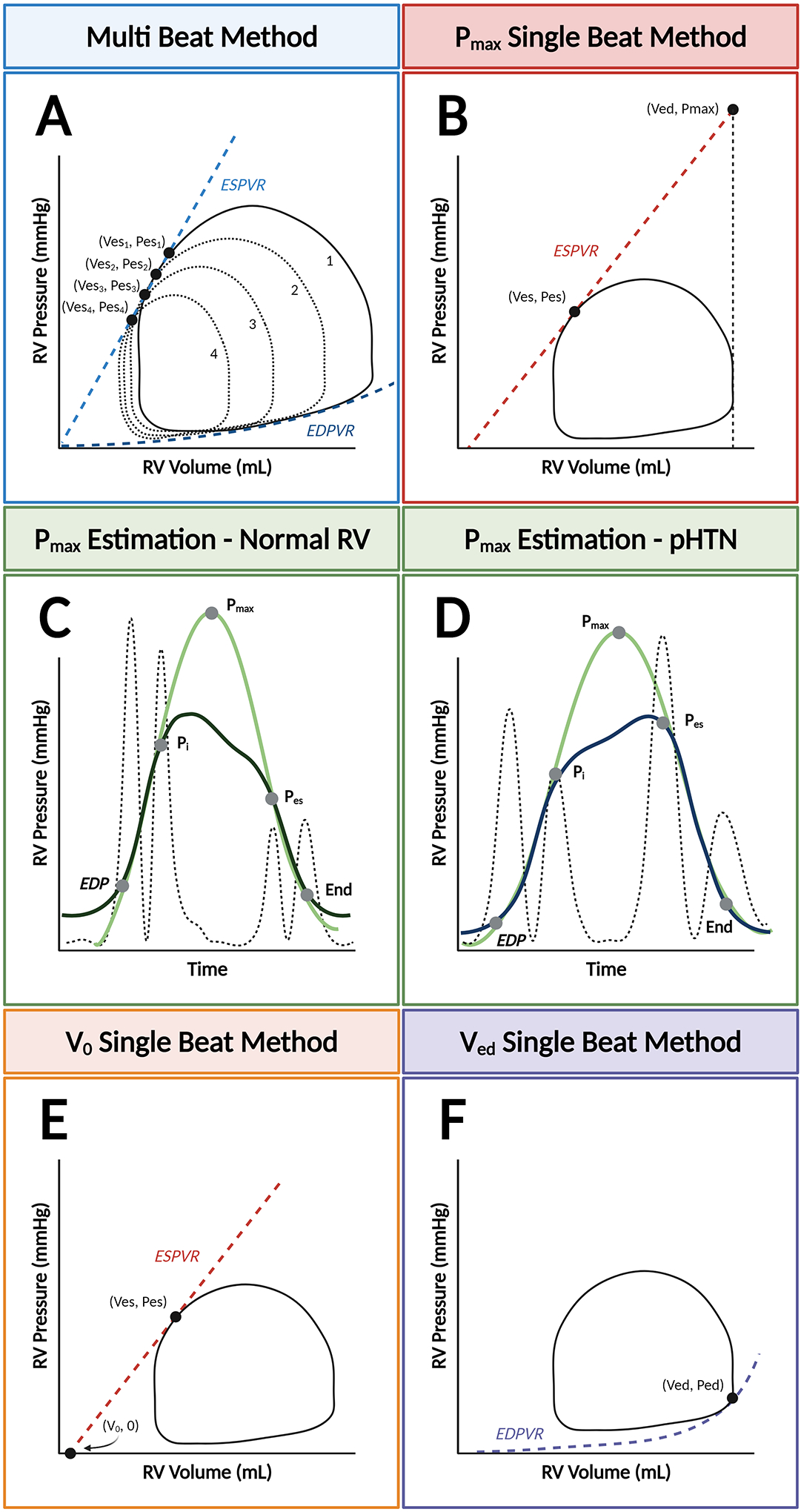
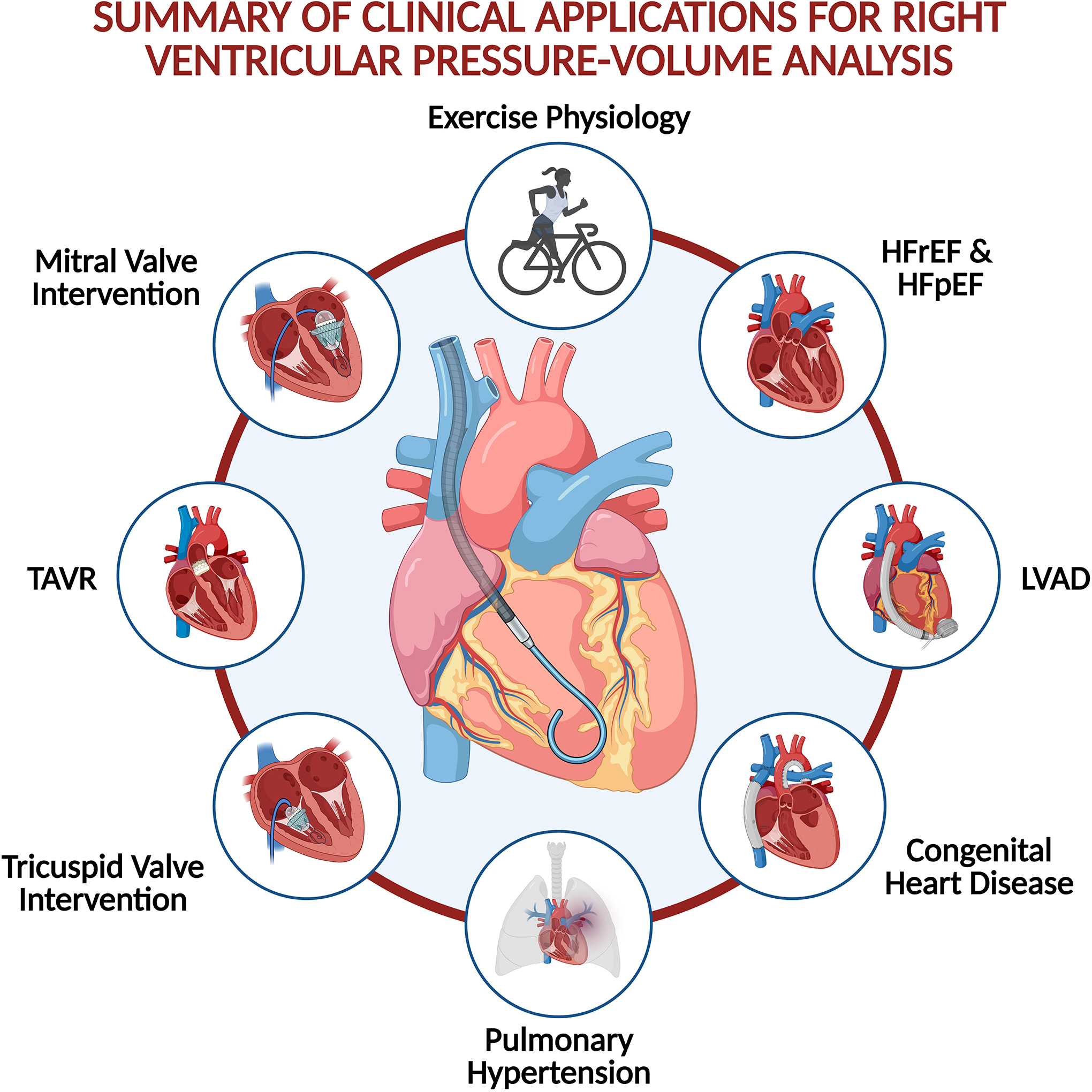
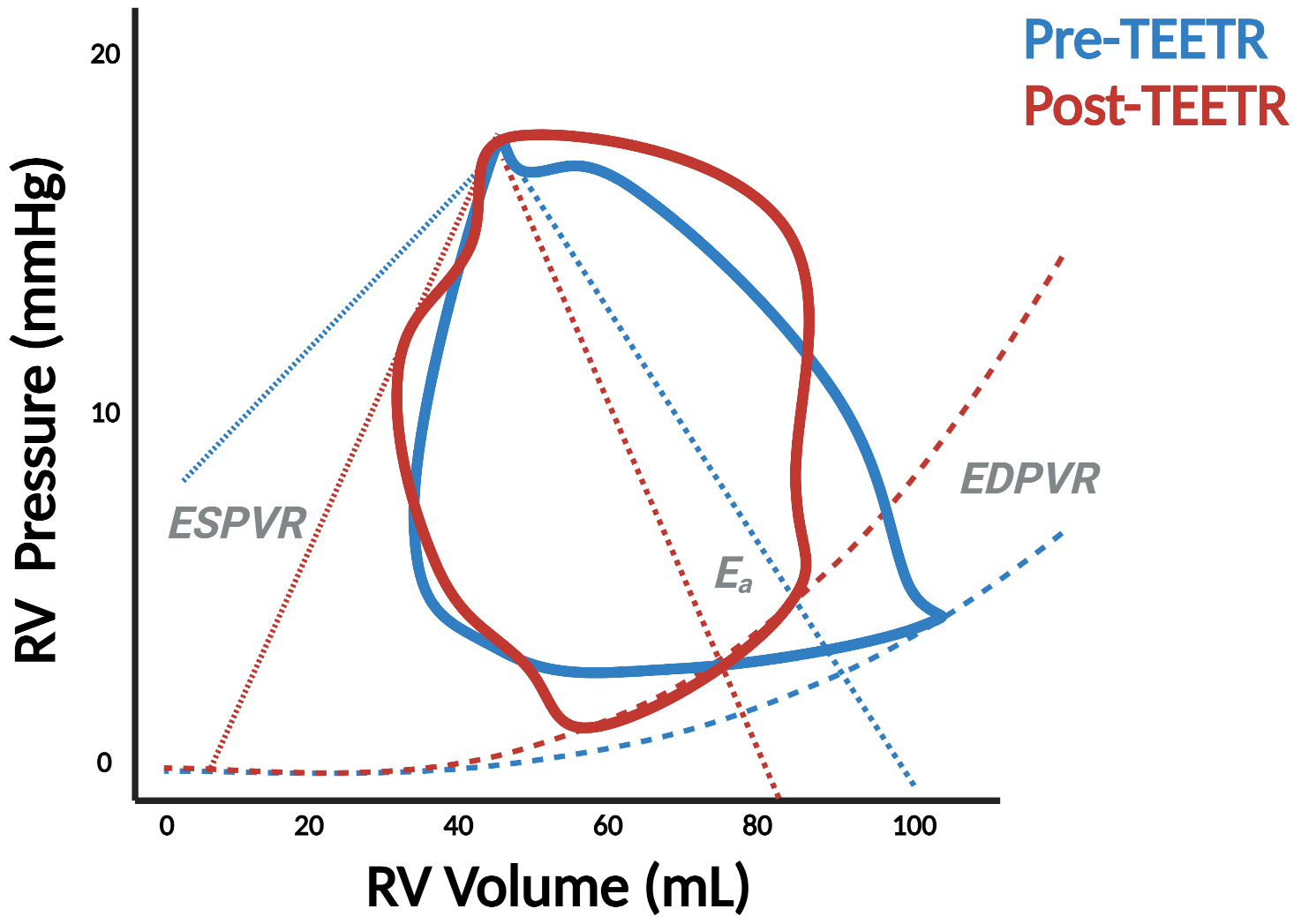
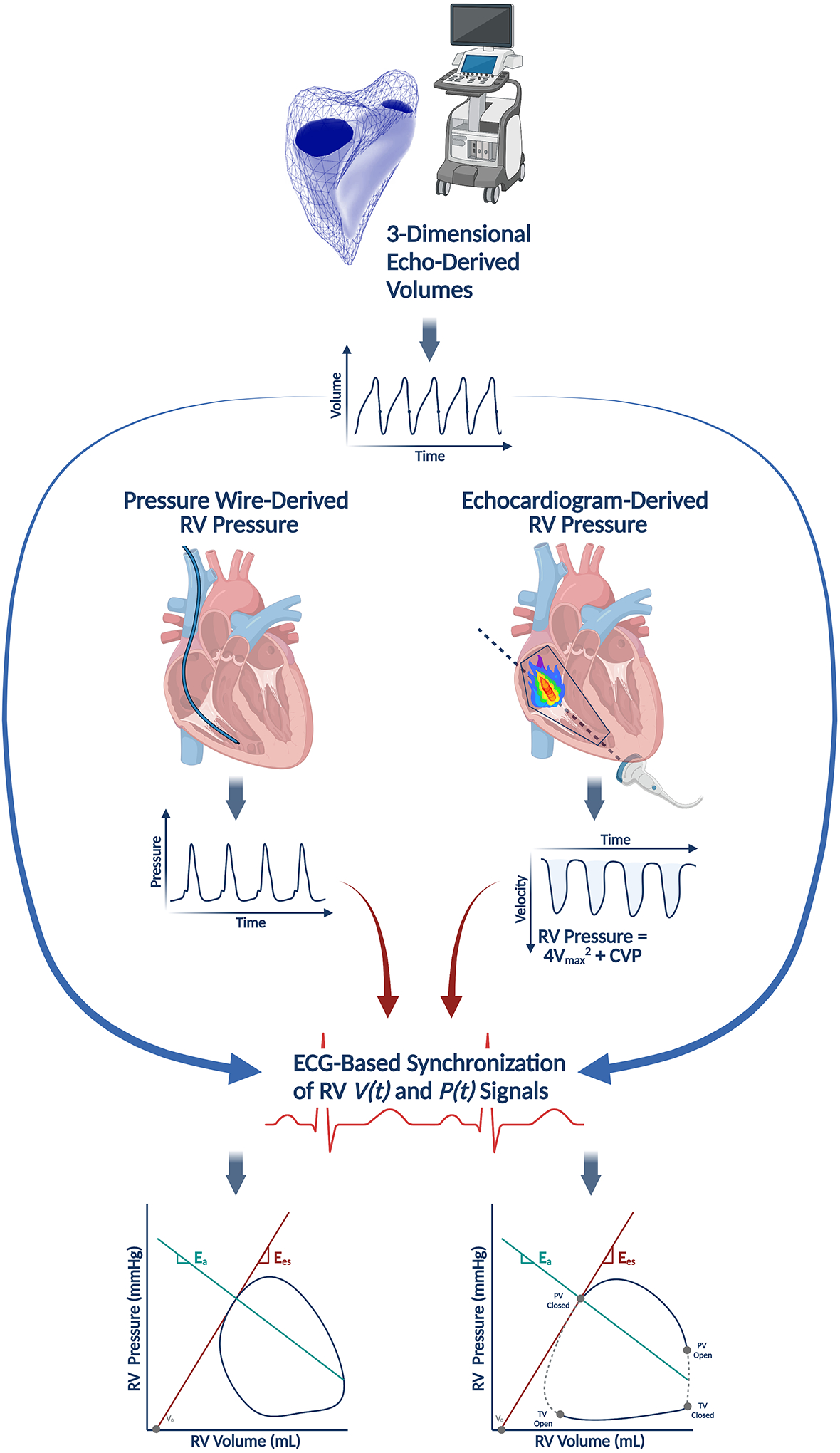
Right ventricular pressure-volume (PV) analysis characterizes ventricular systolic and diastolic properties independent of loading conditions like volume status and afterload. While long-considered the gold-standard method for quantifying myocardial chamber performance, it was traditionally only performed in highly specialized research settings. With recent advances in catheter technology and more sophisticated approaches to analyze PV data, it is now more commonly used in a variety of clinical and research settings. Herein, we review the basic techniques for PV loop measurement, analysis, and interpretation with the aim of providing readers with a deeper understanding of the strengths and limitations of PV analysis. In the second half of the review, we detail key scenarios in which right ventricular PV analysis has influenced our understanding of clinically relevant topics and where the technique can be applied to resolve additional areas of uncertainty. All told, PV analysis has an important role in advancing our understanding of right ventricular physiology and its contribution to cardiovascular function in health and disease.
Keywords: heart failure; hemodynamics; pulmonary circulation; ventricular function, right.
Figures
References
-
- Sanz J, Sánchez-Quintana D, Bossone E, Bogaard HJ and Naeije R. Anatomy, Function, and Dysfunction of the Right Ventricle: JACC State-of-the-Art Review. Journal of the American College of Cardiology. 2019;73:1463–1482. - PubMed
-
- Brener MI, Burkhoff D and Sunagawa K. Effective Arterial Elastance in the Pulmonary Arterial Circulation: Derivation, Assumptions, and Clinical Applications. Circ Heart Fail. 2020;13:e006591. - PubMed
-
- Vonk-Noordegraaf A and Westerhof N. Describing right ventricular function. European Respiratory Journal. 2013;41:1419–1423. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
