

Ultrasound-guided erector spinae plane catheter versus video-assisted paravertebral catheter placement in minimally invasive thoracic surgery: comparing continuous infusion analgesic techniques on early quality of recovery, respiratory function and chronic persistent surgical pain: study protocol for a double-blinded randomised controlled trial
- PMID: 34963493
- PMCID: PMC8715598
- DOI: 10.1186/s13063-021-05863-9
Ultrasound-guided erector spinae plane catheter versus video-assisted paravertebral catheter placement in minimally invasive thoracic surgery: comparing continuous infusion analgesic techniques on early quality of recovery, respiratory function and chronic persistent surgical pain: study protocol for a double-blinded randomised controlled trial
Abstract
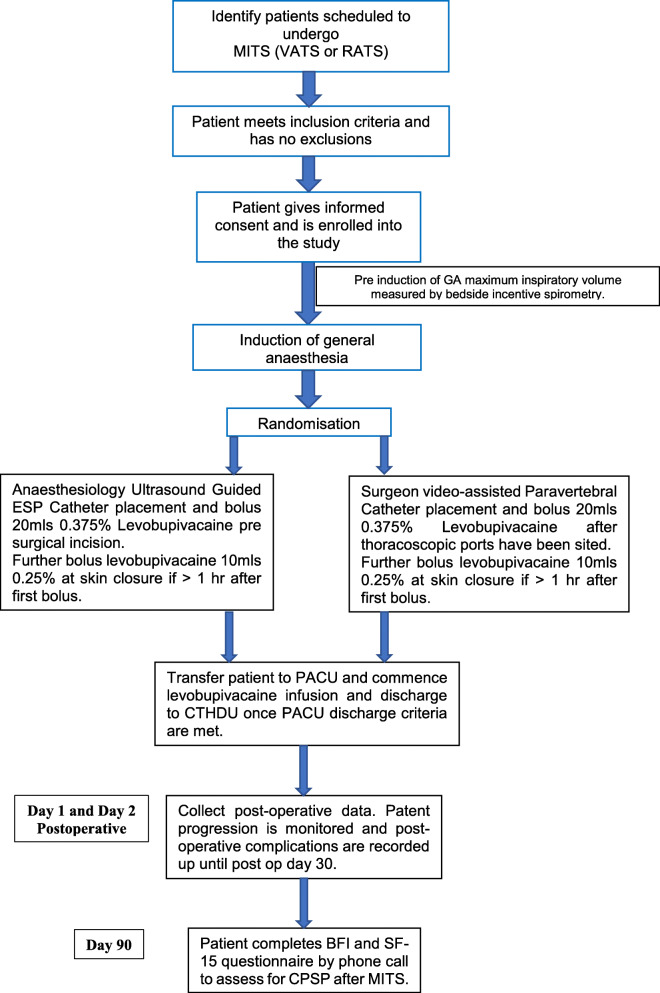
Background: Compared to conventional thoracotomy, minimally invasive thoracic surgery (MITS) can reduce postoperative pain, reduce tissue trauma and contribute to better recovery. However, it still causes significant acute postoperative pain. Truncal regional anaesthesia techniques such as paravertebral and erector spinae blocks have shown to contribute to postoperative analgesia after MITS. Satisfactory placement of an ultrasound-guided thoracic paravertebral catheter can be technically challenging compared to an ultrasound-guided erector spinae catheter. However, in MITS, an opportunity arises for directly visualised placement of a paravertebral catheter by the surgeon under thoracoscopic guidance. Alongside with thoracic epidural, a paravertebral block is considered the "gold standard" of thoracic regional analgesic techniques. To the best of our knowledge, there are no randomised controlled trials comparing surgeon-administered paravertebral catheter and anaesthesiologist-assisted erector spinae catheter for MITS in terms of patient-centred outcomes such as quality of recovery.
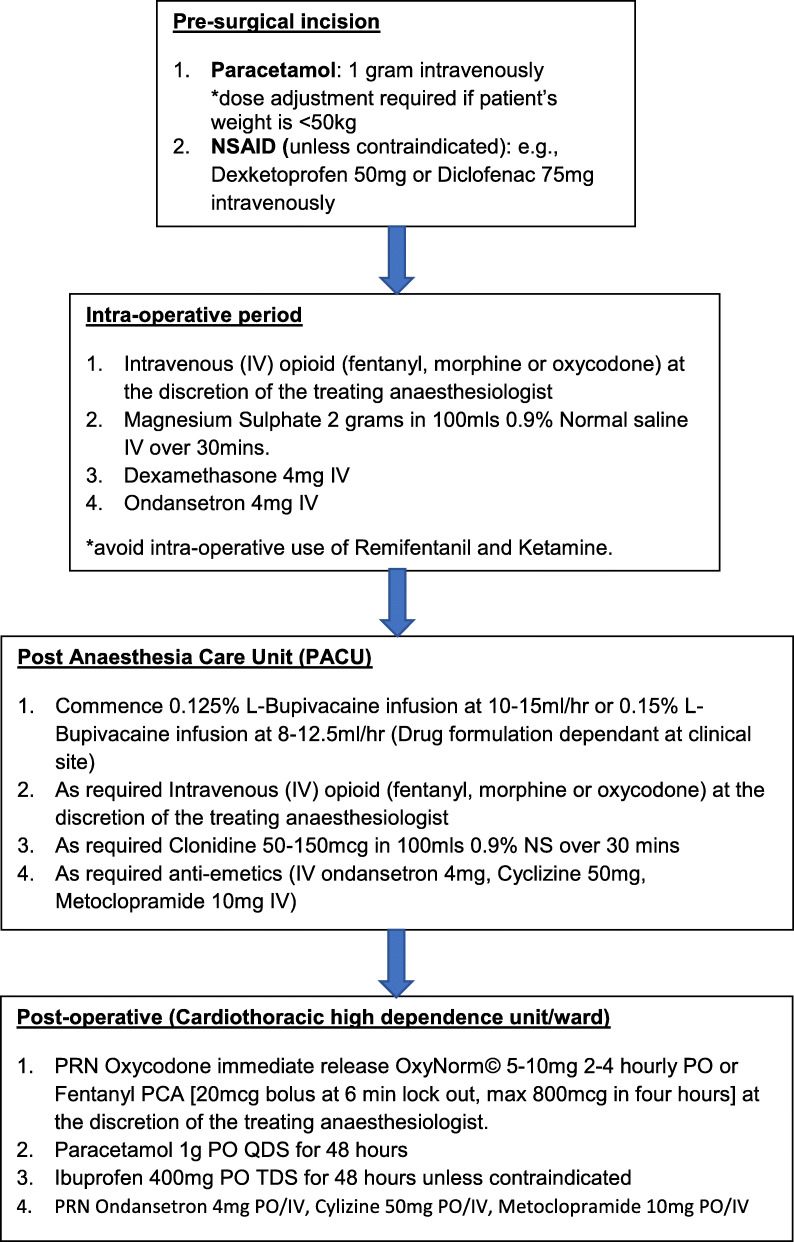
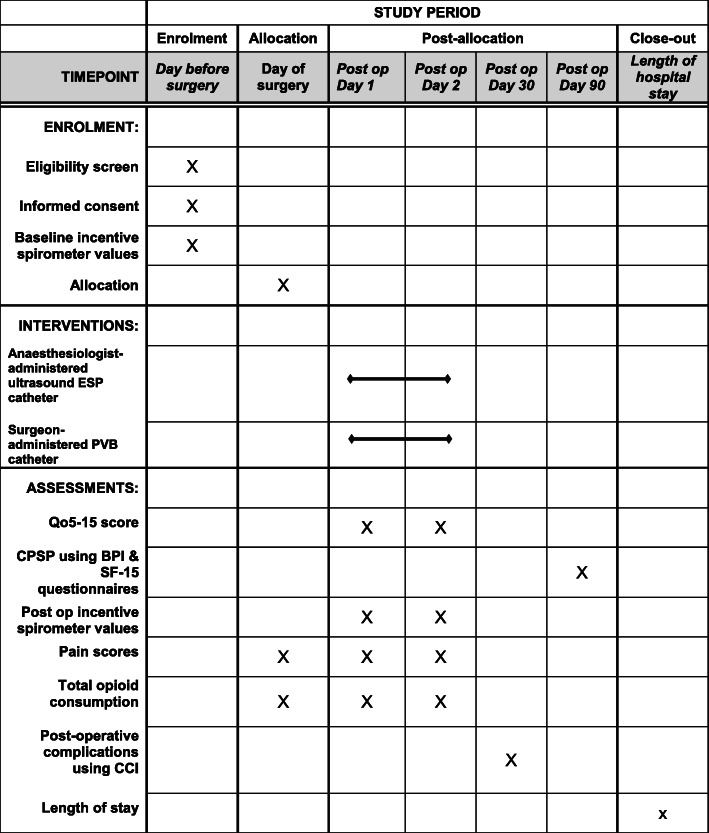
Methods: This trial will be a prospective, double-blinded randomised controlled trial. A total of 80 eligible patients will be randomly assigned to receive either an anaesthesiologist-assisted ultrasound-guided erector spinae catheter or a surgeon-assisted video-assisted paravertebral catheter, in a 1:1 ratio following induction of general anaesthesia for minimally assisted thoracic surgery. Both groups will receive the same standardised analgesia protocol for both intra- and postoperative periods. The primary outcome is defined as Quality of Recovery (QoR-15) score between the two groups at 24 h postoperative. Secondary outcomes include assessment of chronic persistent surgical pain (CPSP) at 3 months postoperative using the Brief Pain Inventory (BPI) Short Form and Short Form McGill (SF-15) questionnaires, assessment of postoperative pulmonary function, area under the curve for Verbal Rating Score for pain at rest and on deep inspiration versus time over 48 h, total opioid consumption over 48 h, QoR-15 at 48 h, and postoperative complications and morbidity as measured by the Comprehensive Complication Index.
Discussion: Despite surgical advancements in thoracic surgery, severe acute postoperative pain following MITS is still prevailing. This study will provide recommendations about the efficacy of an anaesthesia-administered ultrasound-guided erector spinae catheter or surgeon-administered, video-assisted paravertebral catheter techniques for early quality of recovery following MITS.
Trial registration: ClinicalTrials.gov NCT04729712 . Registered on 28 January 2021. All items from the World Health Organization Trial Registration Data Set have been included.
Keywords: Chronic persistent surgical pain; Erector spinae catheter; Minimal invasive thoracic surgery; Paravertebral catheter; Quality of recovery; Randomised controlled trial.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Ultrasound-guided, continuous erector spinae plane (ESP) block in minimally invasive thoracic surgery-comparing programmed intermittent bolus (PIB) vs continuous infusion on quality of recovery and postoperative respiratory function: a double-blinded randomised controlled trial.Trials. 2022 Sep 21;23(1):792. doi: 10.1186/s13063-022-06726-7. Trials. 2022. PMID: 36131308 Free PMC article. Clinical Trial.
-
Postoperative recovery with continuous erector spinae plane block or video-assisted paravertebral block after minimally invasive thoracic surgery: a prospective, randomised controlled trial.Br J Anaesth. 2023 Jan;130(1):e137-e147. doi: 10.1016/j.bja.2022.07.051. Epub 2022 Sep 13. Br J Anaesth. 2023. PMID: 36109206 Clinical Trial.
-
Continuous erector spinae plane block versus thoracic epidural analgesia in video-assisted thoracic surgery: a study protocol for a prospective randomized open label non-inferiority trial.Trials. 2021 May 4;22(1):321. doi: 10.1186/s13063-021-05275-9. Trials. 2021. PMID: 33947442 Free PMC article.
-
Efficacy of erector spinae plane block for analgesia in breast surgery: a systematic review and meta-analysis.Anaesthesia. 2021 Mar;76(3):404-413. doi: 10.1111/anae.15164. Epub 2020 Jul 1. Anaesthesia. 2021. PMID: 32609389
-
Analgesic effect of erector spinae plane block in adults undergoing laparoscopic cholecystectomy: a systematic review and meta-analysis of randomized controlled trials.BMC Anesthesiol. 2023 Jan 6;23(1):7. doi: 10.1186/s12871-023-01969-6. BMC Anesthesiol. 2023. PMID: 36609244 Free PMC article.
Cited by
-
Efficacy of Intrathoracic Intercostal Nerve Block on Postoperative Acute and Chronic Pains of Patients Undergoing Video-Assisted Thoracoscopic Surgery.J Pain Res. 2022 Aug 6;15:2273-2281. doi: 10.2147/JPR.S369042. eCollection 2022. J Pain Res. 2022. PMID: 35967470 Free PMC article. Clinical Trial.
-
Ultrasound-guided, continuous erector spinae plane (ESP) block in minimally invasive thoracic surgery-comparing programmed intermittent bolus (PIB) vs continuous infusion on quality of recovery and postoperative respiratory function: a double-blinded randomised controlled trial.Trials. 2022 Sep 21;23(1):792. doi: 10.1186/s13063-022-06726-7. Trials. 2022. PMID: 36131308 Free PMC article. Clinical Trial.
-
Bilevel opposite direction ESP block with indwelling catheter in the management of severe lung cancer pain.Interv Pain Med. 2022 Sep 6;1(4):100144. doi: 10.1016/j.inpm.2022.100144. eCollection 2022 Dec. Interv Pain Med. 2022. PMID: 39238858 Free PMC article.
-
Analgesic Effectiveness of Ultrasound-Guided Unilateral Erector Spine Block Versus Paravertebral Block for Postoperative Management Among Adult Patients Undergoing Upper Abdominal Surgery: A Prospective Cohort Study.Ann Med Surg (Lond). 2025 Mar 18;87(5):2568-2575. doi: 10.1097/MS9.0000000000003192. eCollection 2025 May. Ann Med Surg (Lond). 2025. PMID: 40337402 Free PMC article.
-
The effects of different analgesic methods on chronic pain in patients undergoing video-assisted thoracoscopic surgery.Wideochir Inne Tech Maloinwazyjne. 2023 Mar;18(1):157-165. doi: 10.5114/wiitm.2022.120572. Epub 2022 Oct 22. Wideochir Inne Tech Maloinwazyjne. 2023. PMID: 37064570 Free PMC article.
References
-
- Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, Brunelli A, Cerfolio RJ, Gonzalez M, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS(R)) Society and the European Society of Thoracic Surgeons (ESTS) Eur J Cardiothorac Surg. 2019;55(1):91–115. doi: 10.1093/ejcts/ezy301. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
