

Optic neuropathy secondary to granulomatosis with polyangiitis in a patient with Graves' disease: a case report
- PMID: 34963497
- PMCID: PMC8715570
- DOI: 10.1186/s13256-021-03207-4
Optic neuropathy secondary to granulomatosis with polyangiitis in a patient with Graves' disease: a case report
Abstract
Background: Dysthyroid optic neuropathy is the most commonly suspected diagnosis of optic neuropathy in Graves' patients; however, other causes need to be ruled out. We present a unique case of optic neuropathy secondary to hypertrophic pachymeningitis with antineutrophil cytoplasmic antibody-associated vasculitis, which was suspected to be antithyroid drug related.
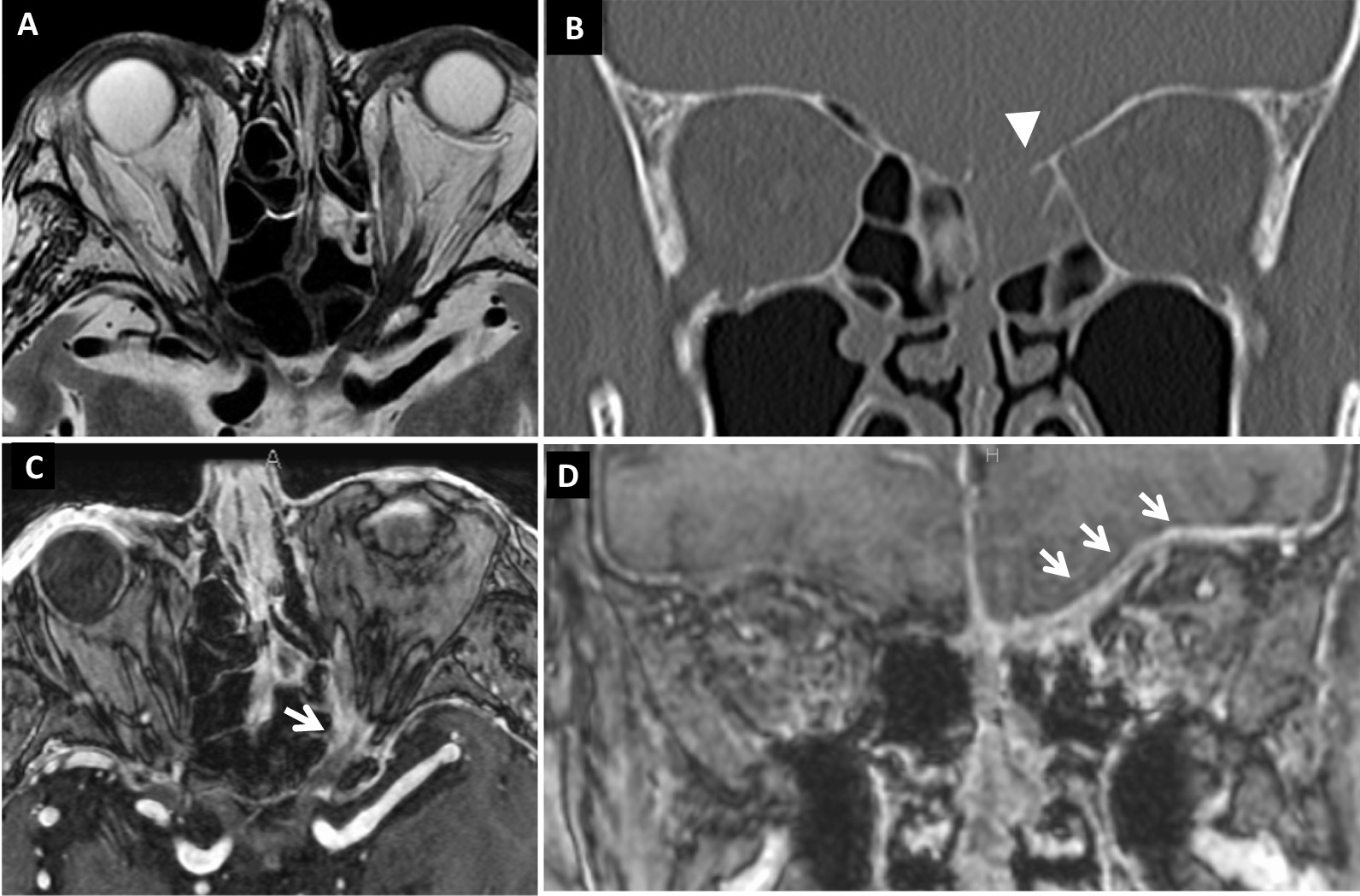
Case presentation: A 79-year-old Japanese male presented with acute visual loss in the left eye. He had a 24-year history of Graves' disease and was taking methimazole. Best-corrected visual acuity was 0.8 in the right eye and light perception in the left eye, and relative afferent pupillary defect in the left eye was seen. Ocular movement was normal, and there were no findings explaining visual loss in intermediate optic media and fundus in the left eye. Contrast-enhanced magnetic resonance imaging demonstrated thickened dura mater. Tests for myeloperoxidase-antineutrophil cytoplasmic antibody, proteinuria, and hematuria were positive; pulmonary nodule lesions and a blood clot in the left lower leg were also found. After excluding the presence of diseases that could lead to hypertrophic pachymeningitis, we diagnosed optic neuropathy due to hypertrophic pachymeningitis with granulomatosis with polyangiitis-a subtype of antineutrophil cytoplasmic antibody-associated vasculitis. Since he had history of using methimazole, antineutrophil cytoplasmic antibody-associated vasculitis was considered as drug related. We started high-dosage steroid pulse therapy followed by 1 mg/kg body weight daily of oral prednisolone, and subsequently tapered. Methimazole was stopped. Best-corrected visual acuity recovered to 0.9, 2 weeks after starting treatment. Though myeloperoxidase-antineutrophil cytoplasmic antibody remained negative, the symptom relapsed 6 months after treatment initiation. We gave a second high-dose steroid pulse therapy followed by prednisolone tapered together with methotrexate. Remission remained, and using 4 mg/week methotrexate without prednisolone, myeloperoxidase-antineutrophil cytoplasmic antibody was kept within the normal limit until now, 4 years after onset.
Conclusion: We present a case of optic neuropathy with hypertrophic pachymeningitis related to antineutrophil cytoplasmic antibody-associated vasculitis, which was suspected to be drug related. The patient had good visual recovery after quitting the drug and receiving immunosuppressive therapy with systemic steroids. Hypertrophic pachymeningitis with antineutrophil cytoplasmic antibody-associated vasculitis related to antithyroid drugs should be considered as a differential diagnosis for optic neuropathy in Graves' patients in whom optic nerve compression is not obvious.
Keywords: Antineutrophil cytoplasmic antibody-associated vasculitis; Drug-induced ANCA-associated vasculitis; Graves’ disease; Hypertrophic pachymeningitis; Myeloperoxidase-antineutrophil cytoplasmic antibody.
© 2021. The Author(s).
Conflict of interest statement
The authors have no financial or nonfinancial competing interests to declare.
Figures

Similar articles
-
Hypertrophic pachymeningitis: significance of myeloperoxidase anti-neutrophil cytoplasmic antibody.Brain. 2014 Feb;137(Pt 2):520-36. doi: 10.1093/brain/awt314. Epub 2013 Nov 22. Brain. 2014. PMID: 24271323
-
Hypertrophic pachymeningitis in eosinophilic granulomatosis with polyangiitis.Mod Rheumatol Case Rep. 2022 Jan 7;6(1):80-82. doi: 10.1093/mrcr/rxab009. Mod Rheumatol Case Rep. 2022. PMID: 34480185
-
The Successful Treatment of Myeloperoxidase Antineutrophil Cytoplasmic Antibody-positive Hypertrophic Pachymeningitis in Patients with the Limited Form of Granulomatosis with Polyangiitis Using Methotrexate: Two Case Reports.Intern Med. 2017;56(8):959-965. doi: 10.2169/internalmedicine.56.7742. Epub 2017 Apr 15. Intern Med. 2017. PMID: 28420847 Free PMC article.
-
Hypertrophic pachymeningitis in ANCA-associated vasculitis: Clinical and immunopathological features and insights.Autoimmun Rev. 2023 Jun;22(6):103338. doi: 10.1016/j.autrev.2023.103338. Epub 2023 Apr 14. Autoimmun Rev. 2023. PMID: 37062439 Review.
-
[Case report of Wegener's granulomatosis presenting with multiple cranial nerve palsy and hypertrophic cranial pachymeningitis].Rinsho Shinkeigaku. 2007 Feb-Mar;47(2-3):85-9. Rinsho Shinkeigaku. 2007. PMID: 17511274 Review. Japanese.
Cited by
-
Optic neuropathy as an early manifestation of granulomatosis with polyangiitis: a case report and literature review.Front Med (Lausanne). 2025 Feb 18;12:1515622. doi: 10.3389/fmed.2025.1515622. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40041467 Free PMC article.
-
Granulomatosis With Polyangiitis in Untreated Graves' Disease: A Rare Event.Cureus. 2022 Sep 29;14(9):e29742. doi: 10.7759/cureus.29742. eCollection 2022 Sep. Cureus. 2022. PMID: 36340518 Free PMC article.
References
-
- McKeag D, Lane C, Lazarus JH, Baldeschi L, Boboridis K, Dickinson AJ, Hullo AI, Kahaly G, Krassas G, Marcocci C, et al. Clinical features of dysthyroid optic neuropathy: a European Group on Graves' Orbitopathy (EUGOGO) survey. Br J Ophthalmol. 2007;91(4):455–458. doi: 10.1136/bjo.2006.094607. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
