

Individual-level barriers to bariatric surgery from patient and provider perspectives: A qualitative study
- PMID: 34963509
- PMCID: PMC9218004
- DOI: 10.1016/j.amjsurg.2021.12.022
Individual-level barriers to bariatric surgery from patient and provider perspectives: A qualitative study
Abstract
Background: Less than 1% adults in the United States who meet body mass index criteria undergo bariatric surgery. Our objective was to identify patient and provider perceptions of individual-level barriers to undergoing bariatric surgery.
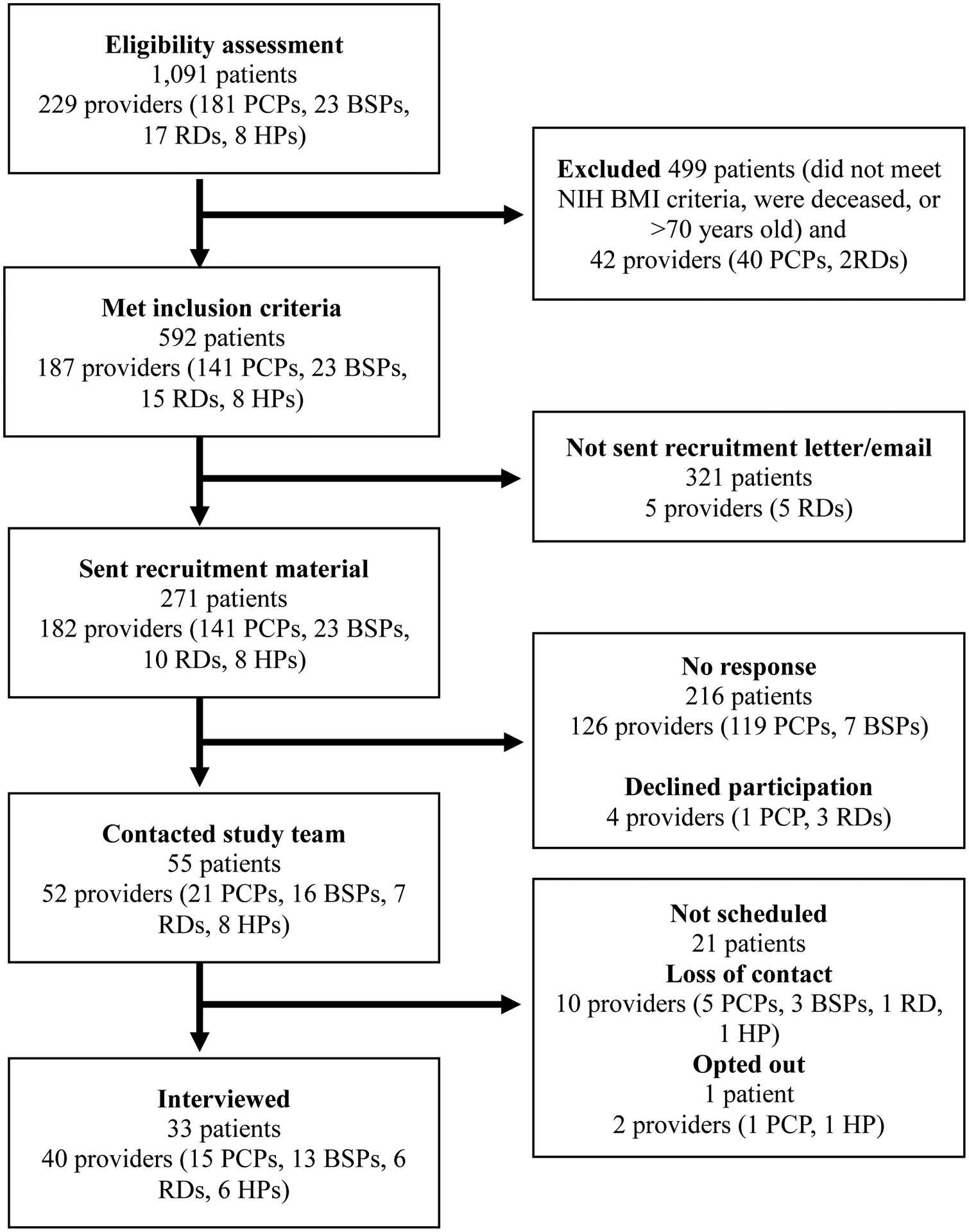
Methods: Adults with severe obesity and obesity care providers described their experiences with the bariatric surgery care process in semi-structured interviews. Using conventional content analysis, individual-level barriers were identified within Andersen's Behavioral Model of Health Services Use.
Results: Of the 73 individuals interviewed, 36 (49%) were female, and 15 (21%) were non-white. Six individual-level barriers were identified: fear of surgery, fear of lifestyle change, perception that weight had not reached its "tipping point," concerns about dietary changes, lack of social support, and patient characteristics influencing referral.
Conclusions: Patient and provider education should address patient fears of surgery and the belief that surgery is a "last resort." Bariatric surgery programs should strengthen social support networks for patients.
Keywords: Bariatric surgery; Individual-level barriers; Patient barriers; Patient perceptions; Provider perceptions.
Published by Elsevier Inc.
Figures
References
-
- Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric-metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial. Lancet. 2015;386(9997):964–973. 10.1016/s0140-6736(15)00075-6 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
