

Utility of Age-adjusted Charlson Comorbidity Index as a Predictor of Need for Invasive Mechanical Ventilation, Length of Hospital Stay, and Survival in COVID-19 Patients
- PMID: 34963715
- PMCID: PMC8664016
- DOI: 10.5005/jp-journals-10071-23946
Utility of Age-adjusted Charlson Comorbidity Index as a Predictor of Need for Invasive Mechanical Ventilation, Length of Hospital Stay, and Survival in COVID-19 Patients
Abstract
Background: Multiple parameters may be used to prognosticate coronavirus disease-2019 (COVID-19) patients, which are often expensive laboratory or radiological investigations. We evaluated the utility of age-adjusted Charlson comorbidity index (CCI) as a predictor of outcome in COVID-19 patients treated with remdesivir.
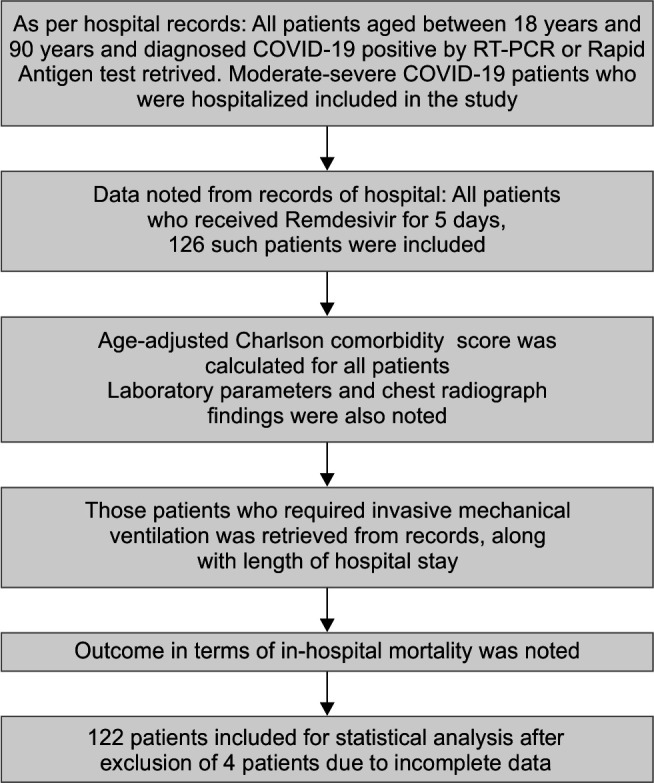
Materials and methods: This was a single-center, retrospective study on 126 COVID-19 patients treated with remdesivir. The age-adjusted CCI, length of hospital stay (LOS), need for invasive mechanical ventilation (IMV), and survival were recorded.
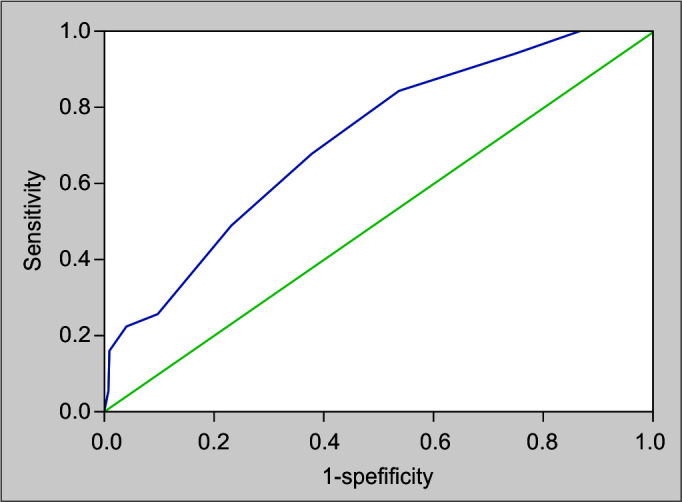
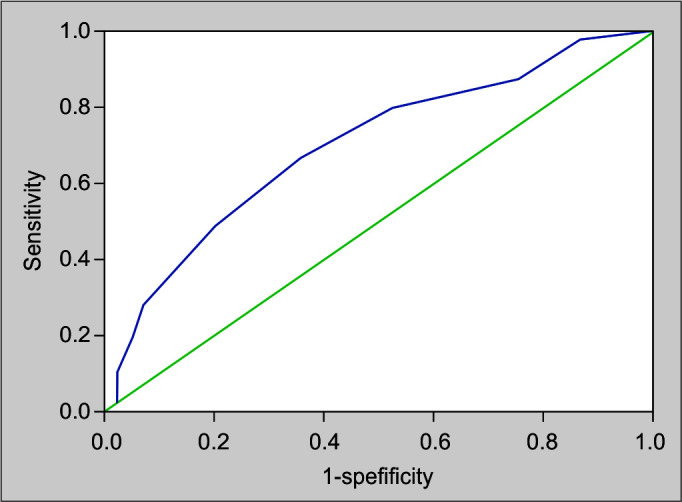
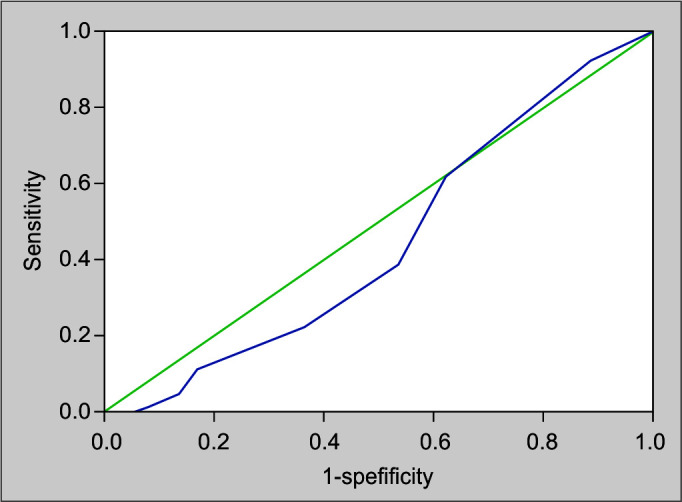
Results: The mean and standard deviation (SD) of age-adjusted CCI were 3.37 and 2.186, respectively. Eighty-six patients (70.5%) had age-adjusted CCI ≤4, and 36 (29.5%) had age-adjusted CCI >4. Among patients with age-adjusted CCI ≤4, 20 (23.3%) required IMV, whereas in those with age-adjusted CCI >4, 19 (52.8%) required IMV (p <0.05, Pearson's chi-square test). In those with age-adjusted CCI ≤4, the mortality was 18.6%, whereas it was 41.7% in patients with age-adjusted CCI >4 (p <0.05, Pearson's chi-square test). The receiver operating curve (ROC) of age-adjusted CCI for predicting the mortality had an area under the curve (AUC) of 0.709, p = 0.001, and sensitivity 68%, specificity 62%, and 95% confidence interval (CI) [0.608, 0.810], for a cutoff score >4. The ROC for age-adjusted CCI for predicting the need for IMV had an AUC of 0.696, p = 0.001, and sensitivity 67%, specificity 63%, and 95% CI [0.594, 0.797], for a cutoff score >4. ROC for age-adjusted CCI as a predictor of prolonged LOS (≥14 days) was insignificant.
Conclusion: In COVID-19 patients, the age-adjusted CCI is an independent predictor of the need for IMV (score >4) and mortality (score >4) but is not useful to predict LOS (CTRI/2020/11/029266).
How to cite this article: Shanbhag V, Arjun NR, Chaudhuri S, Pandey AK. Utility of Age-adjusted Charlson Comorbidity Index as a Predictor of Need for Invasive Mechanical Ventilation, Length of Hospital Stay, and Survival in COVID-19 Patients. Indian J Crit Care Med 2021;25(9):987-991.
Keywords: Age-adjusted Charlson comorbidity index; Coronavirus disease 2019; Invasive mechanical ventilation; Length of hospital stay; Mortality; Remdesivir.
Copyright © 2021; Jaypee Brothers Medical Publishers (P) Ltd.
Conflict of interest statement
Source of support: Nil Conflict of interest: None
Figures
References
LinkOut - more resources
Full Text Sources