

An Approach to Intraoperatively Identify the Coronal Plane Deformities of the Distal Tibia When Treating Tibial Fractures with Intramedullary Nail Fixation: a Retrospective Study
- PMID: 34964267
- PMCID: PMC8867441
- DOI: 10.1111/os.13194
An Approach to Intraoperatively Identify the Coronal Plane Deformities of the Distal Tibia When Treating Tibial Fractures with Intramedullary Nail Fixation: a Retrospective Study
Abstract
Objective: To develop a new approach to intraoperatively identify the presence of coronal plane deformities (both valgus and varus) when treating tibial fractures with closed reduction and intramedullary nail fixation.
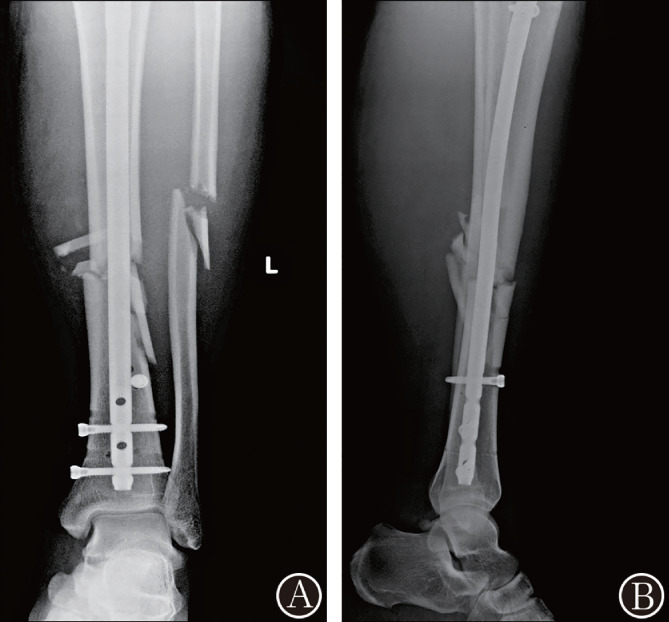
Methods: A retrospective analysis was conducted by enrolling 33 consecutive patients with tibial fractures who received closed reduction and intramedullary nail fixation from January 2018 to January 2019 at our trauma center. Out of the 33 patients, 23 were males and 10 were females and the average age was 41 years (ranging 22 to 69 years of age). Standard anteroposterior and lateral preoperative radiographs were routinely performed. After intraoperatively inserting the tibial intramedullary nail through the standard entry point, the parallel relationship between the distal horizontal interlocking screw and the tibiotalar joint surface on the anteroposterior fluoroscopy was used to determine the occurrence of valgus or varus deformities of the distal tibial fragment. Radiographic and clinical outcomes were analyzed using the average interval from injury to surgery, the lateral distal tibial angle (LDTA) of the unaffected and affected sides, complications and the Olerud-Molander ankle score.
Results: All 33 patients were postoperatively followed for 13 to 25 months (mean 18.7 months). The fractures achieved bone union at an average of 4.3 months (ranging from 3 to 6 months). The total complication rate was 60.6% (20 cases), including four cases that showed deep vein thrombosis, one case showing an infection and delayed union and 15 cases showing slight to moderate anterior knee pain. The postoperative LDTA of the unaffected side measured 87.3° to 89.6 ° (average 88.7° ± 0.8°), and the LDTA of the affected side was 87.5° to 90.4° (average 88.9° ± 1.1°). There was no significant difference between the unaffected and affected sides (t = -1.865, P = 0.068). The intraoperative measurement indicated six cases of valgus angulation and three cases of varus angulation deformities, and all deformities were corrected during surgery. According to the Olerud-Molander ankle score, clinical outcomes demonstrated 22 excellent cases, eight good cases, two fair cases, and one poor case 12 months after surgery.
Conclusion: The parallel relationship between the distal horizontal interlocking screw and tibiotalar joint surface on intraoperative anteroposterior films were able to determine the onset of valgus or varus angulations of the distal tibial fragment in the fracture zone after the tibial intramedullary nail was inserted through the standard entry point.
Keywords: Angulation deformity; Intramedullary nail; Tibia fracture; Valgus; Varus.
© 2021 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures




References
-
- Xue XH, Yan SG, Cai XZ, Shi MM, Lin T. Intramedullary nailing versus plating for extra‐articular distal tibial metaphyseal fracture: a systematic review and meta‐analysis. Injury, 2014, 45: 667–676. - PubMed
-
- Moreschini O, Petrucci V, Cannata R. Insertion of distal locking screws of tibial intramedullary nails: a comparison between the free‐hand technique and the SURESHOT™ distal targeting system. Injury, 2014, 45: 405–407. - PubMed
-
- Ristiniemi J, Flinkkilä T, Hyvönen P, et al. Two‐ring hybrid external fixation of distal tibial fractures: a review of 47 cases. J Trauma, 2007, 62: 174–183. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
