

Anti-EGFR monoclonal antibody plus chemotherapy for treating advanced non-small cell lung cancer: A meta-analysis
- PMID: 34964780
- PMCID: PMC8615333
- DOI: 10.1097/MD.0000000000027954
Anti-EGFR monoclonal antibody plus chemotherapy for treating advanced non-small cell lung cancer: A meta-analysis
Abstract
Background: The use of standard cytotoxic chemotherapy seems to have reached a "treatment plateau". The application of anti-epidermal growth factor receptor (EGFR) monoclonal antibodies (mAbs) is a new strategy for non-small-cell lung cancer (NSCLC) therapy. We aimed to comprehensively assess the efficacy and safety of anti-EGFR-mAbs plus chemotherapy as first-line therapy for advanced NSCLC.
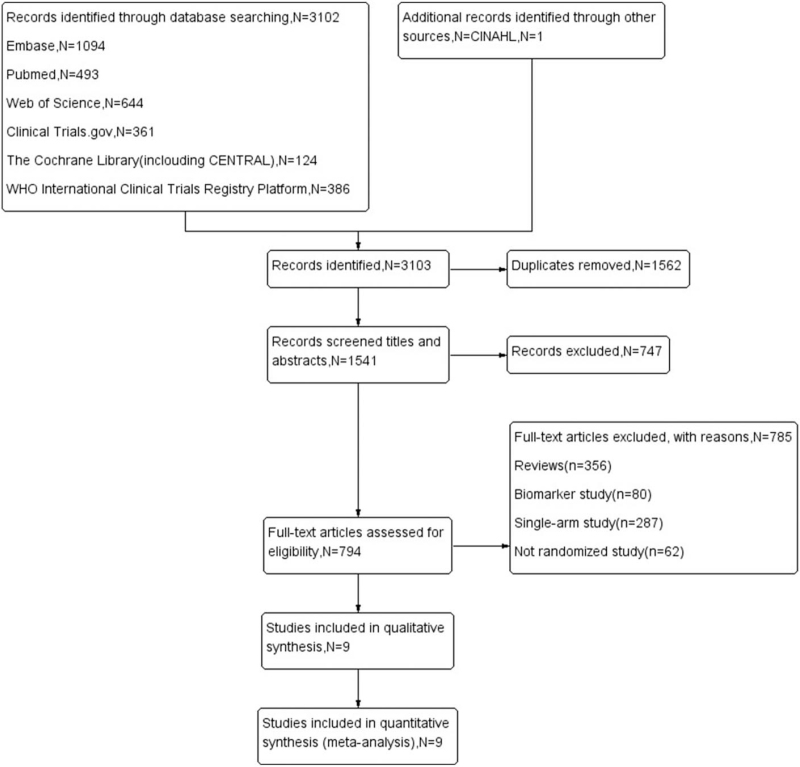
Methods: According to inclusion and exclusion criteria, we conducted a comprehensive literature search of electronic databases. From the included trials, information on overall survival (OS), progression-free survival (PFS), objective response rate (ORR), and adverse events (AEs) was extracted.
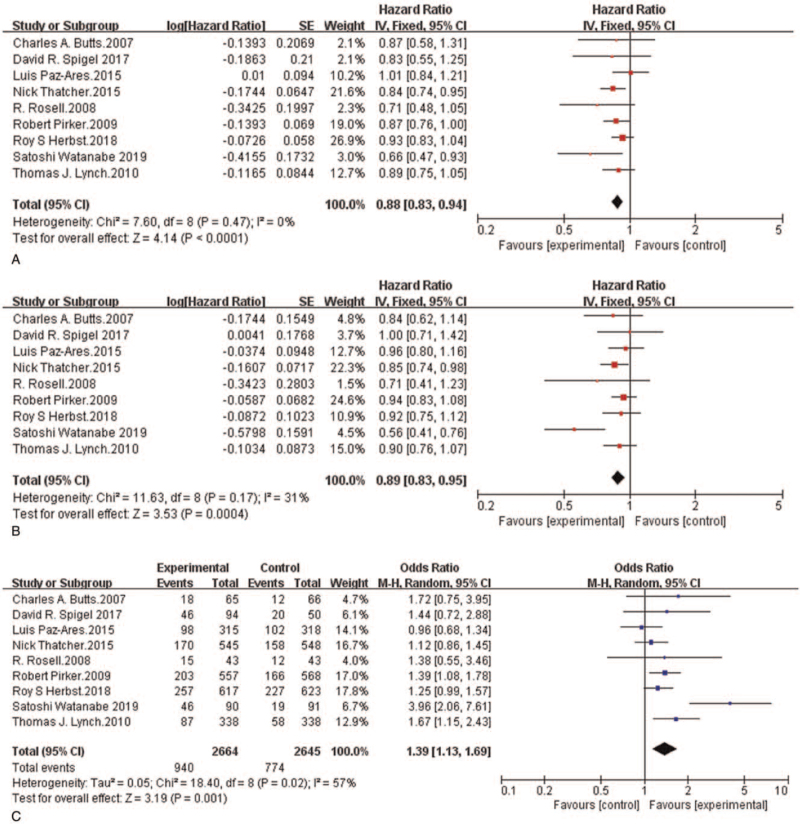
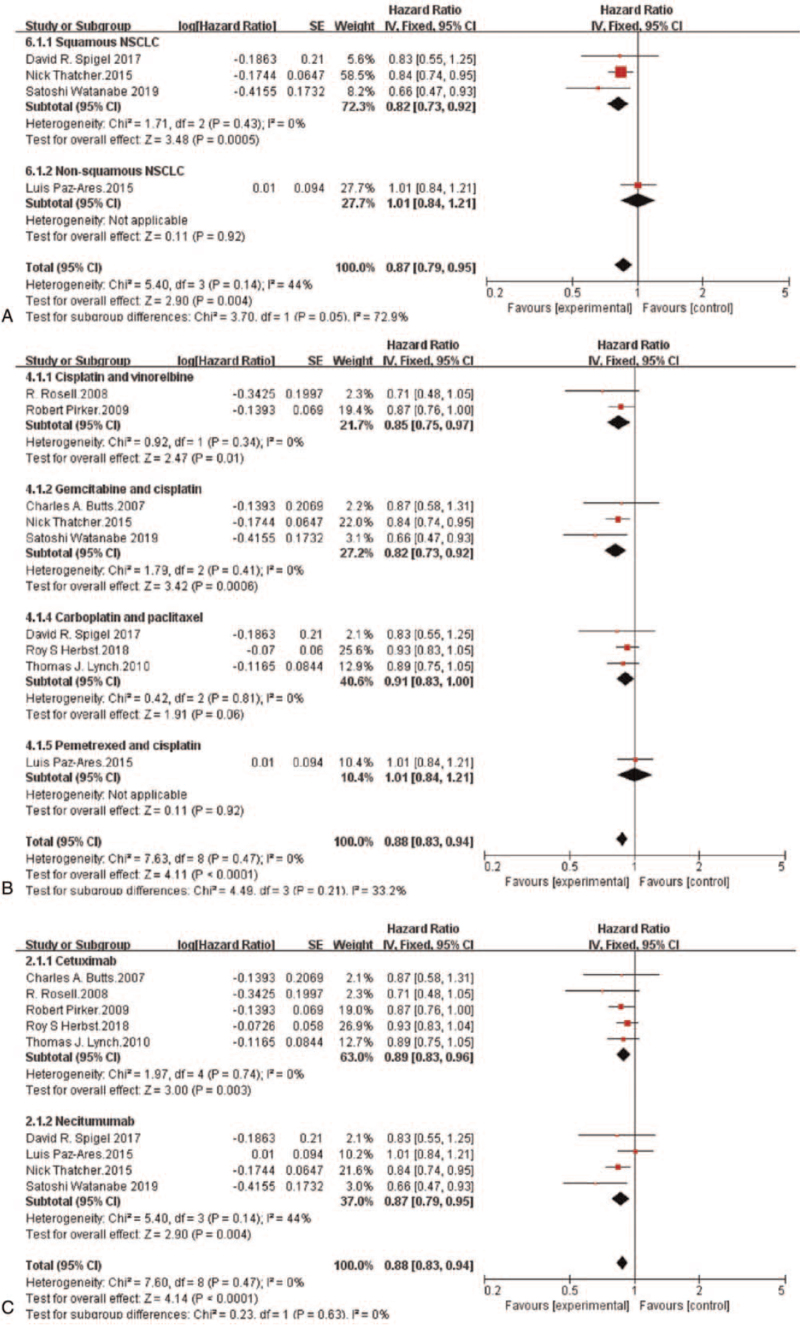
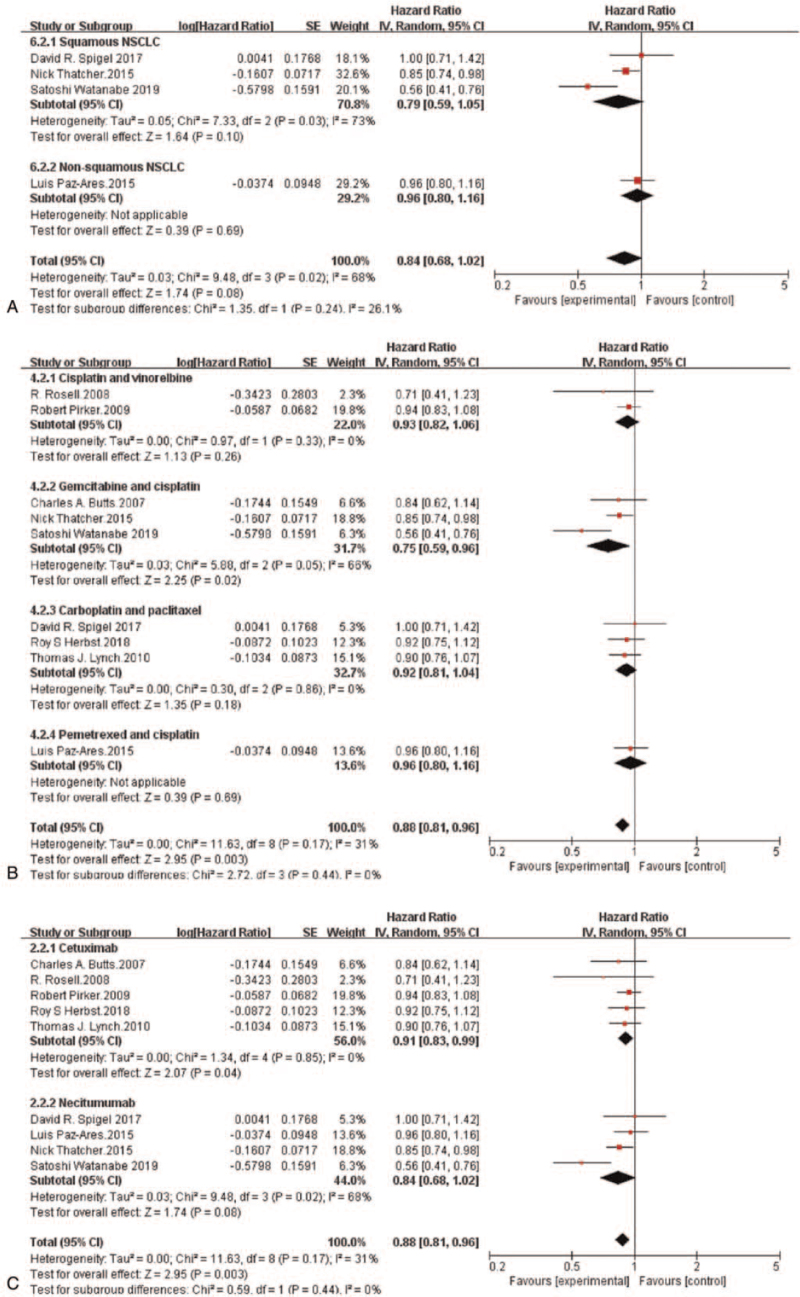
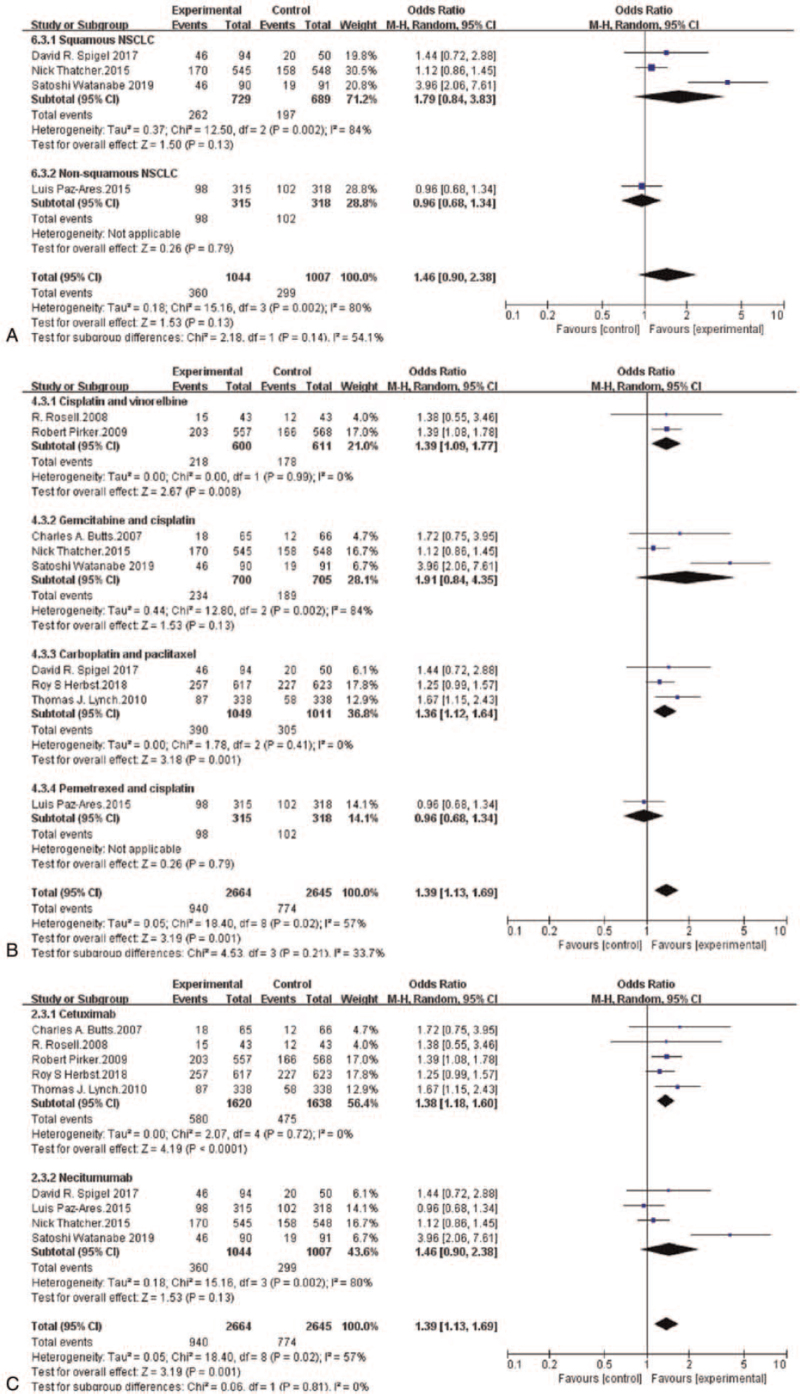
Results: The research showed that compared with chemotherapy alone, anti-EGFR-mAb plus chemotherapy combinations significantly improved OS (HR = 0.88, 95%CI: 0.83-0.94, P < .0001), PFS (HR = 0.89, 95%CI: 0.83-0.95, P = 0.0004) and ORR (OR = 1.39, 95%CI: 1.13-1.69, P = .001). Meta subgroup analyses manifested that the OS of patients with squamous NSCLC treated with anti-EGFR-mAb plus chemotherapy combinations was notably better than that of patients with non-squamous NSCLC treated with the same combinations (HR = 0.82, 95%CI: 0.73-0.92, P = .0005). Compared with the chemotherapy group, combination of chemotherapy and anti-EGFR mAb showed increase in incidences of severe AEs (> = grade 3) that mainly include, leukopenia (OR = 1.53, 95%CI: 1.28-1.82, P < .00001), febrile neutropenia (OR = 1.35, 95%CI: 1.06-1.71, P = .02), hypomagnesemia (OR = 5.68, 95%CI: 3.54-9.10, P < .00001), acneiform rash (OR = 35.88, 95%CI: 17.37-74.10, P < .00001), fatigue (OR = 1.24, 95%CI: 1.02-1.49, P = .03), diarrhea (OR = 1.69, 95%CI: 1.16-2.47, P = .006), and infusion-related reactions (OR = 3.78, 95%CI: 1.93-7.41, P = .0001).
Conclusion: Adding an anti-EGFR-mAb to the standard platinum-based chemotherapy regimens used for the first-line treatment of advanced NSCLC resulted in statistically notable improvements in OS, PFS, and ORR. In particular, anti-EGFR-mAb and chemotherapy combinations achieved greater survival benefits in patients with squamous NSCLC than in those with non-squamous NSCLC. In addition, the safety profile of chemotherapy plus anti-EGFR-mAb combinations was acceptable compared to that of chemotherapy alone.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Stinchcombe TE, Socinski MA. Current treatments for advanced stage non-small cell lung cancer. Proc Am Thorac Soc 2009;6:233–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
