

An Artificial Intelligence-Based Chest X-ray Model on Human Nodule Detection Accuracy From a Multicenter Study
- PMID: 34964851
- PMCID: PMC8717119
- DOI: 10.1001/jamanetworkopen.2021.41096
An Artificial Intelligence-Based Chest X-ray Model on Human Nodule Detection Accuracy From a Multicenter Study
Abstract
Importance: Most early lung cancers present as pulmonary nodules on imaging, but these can be easily missed on chest radiographs.
Objective: To assess if a novel artificial intelligence (AI) algorithm can help detect pulmonary nodules on radiographs at different levels of detection difficulty.
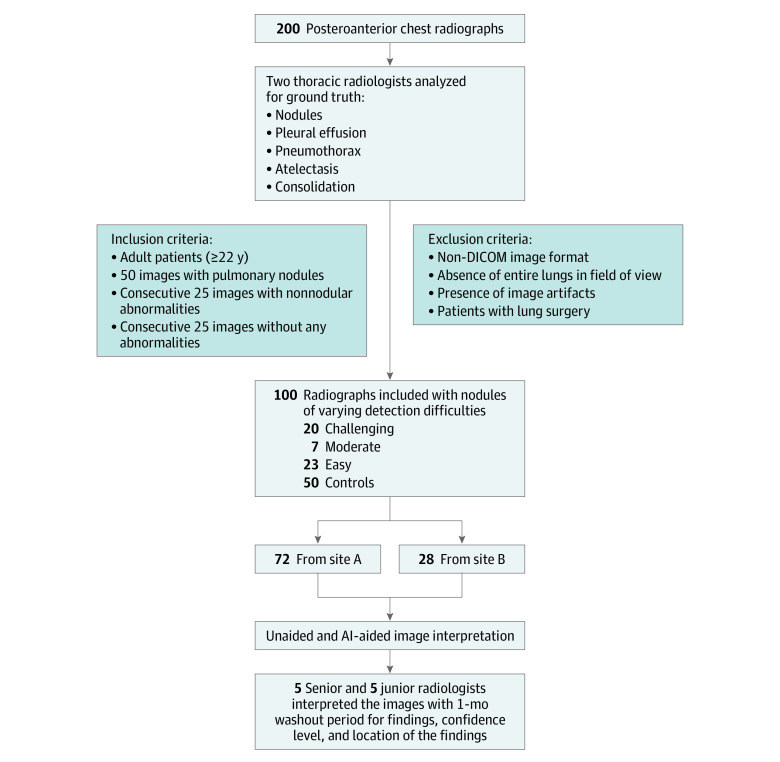
Design, setting, and participants: This diagnostic study included 100 posteroanterior chest radiograph images taken between 2000 and 2010 of adult patients from an ambulatory health care center in Germany and a lung image database in the US. Included images were selected to represent nodules with different levels of detection difficulties (from easy to difficult), and comprised both normal and nonnormal control.
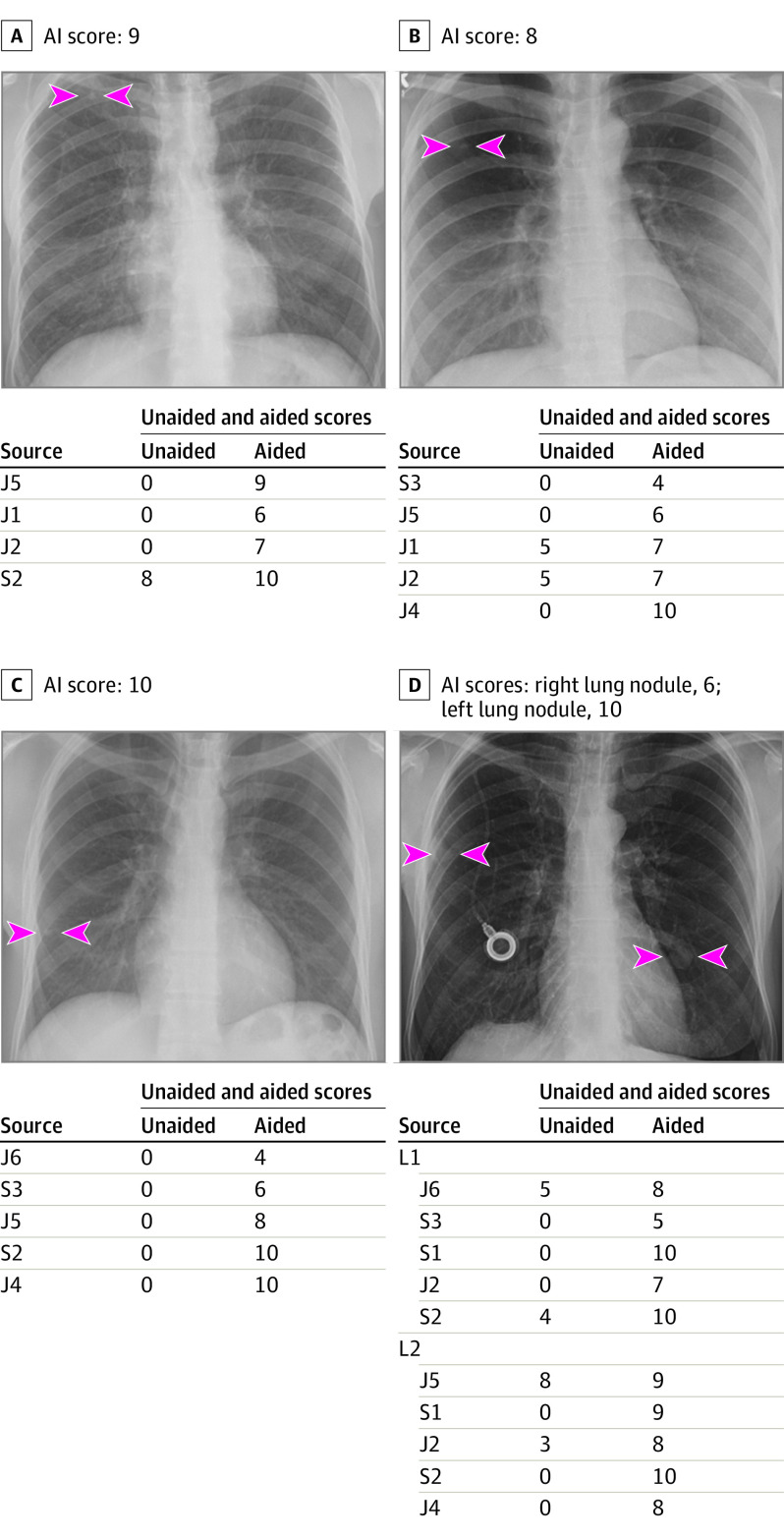
Exposures: All images were processed with a novel AI algorithm, the AI Rad Companion Chest X-ray. Two thoracic radiologists established the ground truth and 9 test radiologists from Germany and the US independently reviewed all images in 2 sessions (unaided and AI-aided mode) with at least a 1-month washout period.
Main outcomes and measures: Each test radiologist recorded the presence of 5 findings (pulmonary nodules, atelectasis, consolidation, pneumothorax, and pleural effusion) and their level of confidence for detecting the individual finding on a scale of 1 to 10 (1 representing lowest confidence; 10, highest confidence). The analyzed metrics for nodules included sensitivity, specificity, accuracy, and receiver operating characteristics curve area under the curve (AUC).
Results: Images from 100 patients were included, with a mean (SD) age of 55 (20) years and including 64 men and 36 women. Mean detection accuracy across the 9 radiologists improved by 6.4% (95% CI, 2.3% to 10.6%) with AI-aided interpretation compared with unaided interpretation. Partial AUCs within the effective interval range of 0 to 0.2 false positive rate improved by 5.6% (95% CI, -1.4% to 12.0%) with AI-aided interpretation. Junior radiologists saw greater improvement in sensitivity for nodule detection with AI-aided interpretation as compared with their senior counterparts (12%; 95% CI, 4% to 19% vs 9%; 95% CI, 1% to 17%) while senior radiologists experienced similar improvement in specificity (4%; 95% CI, -2% to 9%) as compared with junior radiologists (4%; 95% CI, -3% to 5%).
Conclusions and relevance: In this diagnostic study, an AI algorithm was associated with improved detection of pulmonary nodules on chest radiographs compared with unaided interpretation for different levels of detection difficulty and for readers with different experience.
Conflict of interest statement
Figures
References
-
- Tack D, Howarth N. Missed Lung Lesions: Side-by-Side Comparison of Chest Radiography with MDCT. In: Hodler J, Kubik-Huch RA, von Schulthess GK, eds. Diseases of the Chest, Breast, Heart and Vessels 2019-2022: Diagnostic and Interventional Imaging. Springer; 2019:17-26. doi:10.1007/978-3-030-11149-6_2 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
