

Association of Posttraumatic Epilepsy With 1-Year Outcomes After Traumatic Brain Injury
- PMID: 34964854
- PMCID: PMC8717106
- DOI: 10.1001/jamanetworkopen.2021.40191
Association of Posttraumatic Epilepsy With 1-Year Outcomes After Traumatic Brain Injury
Abstract
Importance: Posttraumatic epilepsy (PTE) is a recognized sequela of traumatic brain injury (TBI), but the long-term outcomes associated with PTE independent of injury severity are not precisely known.
Objective: To determine the incidence, risk factors, and association with functional outcomes and self-reported somatic, cognitive, and psychological concerns of self-reported PTE in a large, prospectively collected TBI cohort.
Design, setting, and participants: This multicenter, prospective cohort study was conducted as part of the Transforming Research and Clinical Knowledge in Traumatic Brain Injury study and identified patients presenting with TBI to 1 of 18 participating level 1 US trauma centers from February 2014 to July 2018. Patients with TBI, extracranial orthopedic injuries (orthopedic controls), and individuals without reported injuries (eg, friends and family of participants; hereafter friend controls) were prospectively followed for 12 months. Data were analyzed from January 2020 to April 2021.
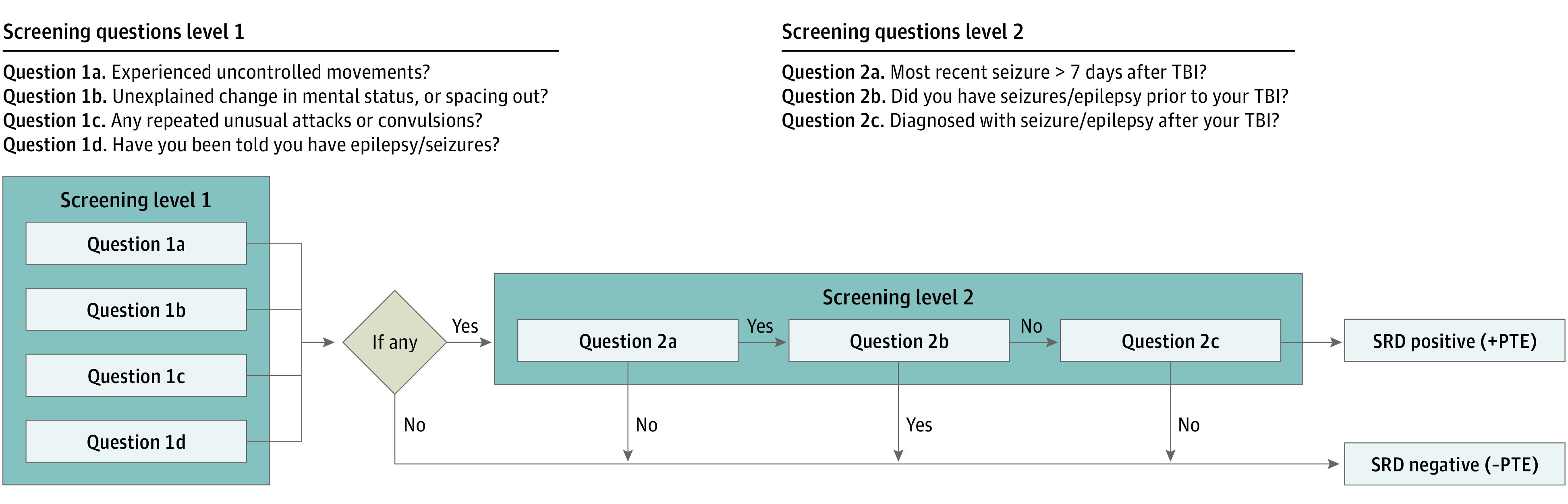
Exposure: Demographic, imaging, and clinical information was collected according to TBI Common Data Elements. Incidence of self-reported PTE was assessed using the National Institute of Neurological Disorders and Stroke Epilepsy Screening Questionnaire (NINDS-ESQ).
Main outcomes and measures: Primary outcomes included Glasgow Outcome Scale Extended, Rivermead Cognitive Metric (RCM; derived from the Rivermead Post Concussion Symptoms Questionnaire), and the Brief Symptom Inventory-18 (BSI).
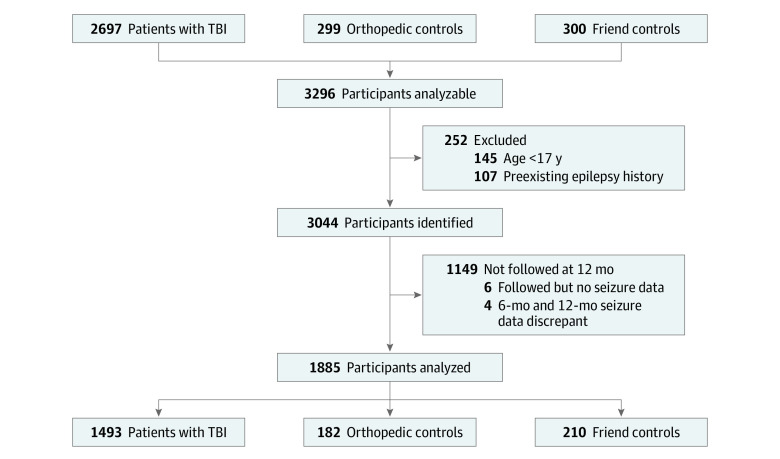
Results: Of 3296 participants identified as part of the study, 3044 met inclusion criteria, and 1885 participants (mean [SD] age, 41.3 [17.1] years; 1241 [65.8%] men and 644 [34.2%] women) had follow-up information at 12 months, including 1493 patients with TBI; 182 orthopedic controls, 210 uninjured friend controls; 41 patients with TBI (2.8%) and no controls had positive screening results for PTE. Compared with a negative screening result for PTE, having a positive screening result for PTE was associated with presenting Glasgow Coma Scale score (8.1 [4.8] vs.13.5 [3.3]; P < .001) as well as with anomalous acute head imaging findings (risk ratio, 6.42 [95% CI, 2.71-15.22]). After controlling for age, initial Glasgow Coma Scale score, and imaging findings, compared with patients with TBI and without PTE, patients with TBI and with positive PTE screening results had significantly lower Glasgow Outcome Scale Extended scores (mean [SD], 6.1 [1.7] vs 4.7 [1.5]; P < .001), higher BSI scores (mean [SD], 50.2 [10.7] vs 58.6 [10.8]; P = .02), and higher RCM scores (mean [SD], 3.1 [2.6] vs 5.3 [1.9]; P = .002) at 12 months.
Conclusions and relevance: In this cohort study, the incidence of self-reported PTE after TBI was found to be 2.8% and was independently associated with unfavorable outcomes. These findings highlight the need for effective antiepileptogenic therapies after TBI.
Conflict of interest statement
Figures
References
-
- Annegers JF. The epidemiology of epilepsy. In: The Treatment of Epilepsy: Principles and Practice. Wyllie E, ed. Wolters Kluwer; 1996:165-172.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
