

A Continuous Correlation Between Residual Tumor Volume and Survival Recommends Maximal Safe Resection in Glioblastoma Patients: A Nomogram for Clinical Decision Making and Reference for Non-Randomized Trials
- PMID: 34966669
- PMCID: PMC8711700
- DOI: 10.3389/fonc.2021.748691
A Continuous Correlation Between Residual Tumor Volume and Survival Recommends Maximal Safe Resection in Glioblastoma Patients: A Nomogram for Clinical Decision Making and Reference for Non-Randomized Trials
Abstract
Objective: The exact role of the extent of resection or residual tumor volume on overall survival in glioblastoma patients is still controversial. Our aim was to create a statistical model showing the association between resection extent/residual tumor volume and overall survival and to provide a nomogram that can assess the survival benefit of individual patients and serve as a reference for non-randomized studies.
Methods: In this retrospective multicenter cohort study, we used the non-parametric Cox regression and the parametric log-logistic accelerated failure time model in patients with glioblastoma. On 303 patients (training set), we developed a model to evaluate the effect of the extent of resection/residual tumor volume on overall survival and created a score to estimate individual overall survival. The stability of the model was validated by 20-fold cross-validation and predictive accuracy by an external cohort of 253 patients (validation set).
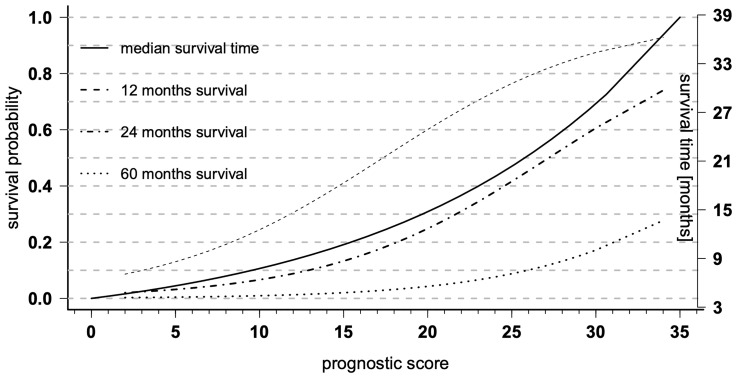
Results: We found a continuous relationship between extent of resection or residual tumor volume and overall survival. Our final accelerated failure time model (pseudo R2 = 0.423; C-index = 0.749) included residual tumor volume, age, O6-methylguanine-DNA-methyltransferase methylation, therapy modality, resectability, and ventricular wall infiltration as independent predictors of overall survival. Based on these factors, we developed a nomogram for assessing the survival of individual patients that showed a median absolute predictive error of 2.78 (mean: 1.83) months, an improvement of about 40% compared with the most promising established models.
Conclusions: A continuous relationship between residual tumor volume and overall survival supports the concept of maximum safe resection. Due to the low absolute predictive error and the consideration of uneven distributions of covariates, this model is suitable for clinical decision making and helps to evaluate the results of non-randomized studies.
Keywords: accelerated failure time; extent of resection; glioblastoma; nomogram; prognostic survival model; reference; residual tumor volume.
Copyright © 2021 Skardelly, Kaltenstadler, Behling, Mäurer, Schittenhelm, Bender, Paulsen, Hedderich, Renovanz, Gempt, Barz, Meyer, Tabatabai and Tatagiba.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Marko NF, Weil RJ, Schroeder JL, Lang FF, Suki D, Sawaya RE. Extent of Resection of Glioblastoma Revisited: Personalized Survival Modeling Facilitates More Accurate Survival Prediction and Supports a Maximum-Safe-Resection Approach to Surgery. J Clin Oncol: Off J Am Soc Clin Oncol (2014) 32:774–82. doi: 10.1200/jco.2013.51.8886 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials