

Analysis of Fibrotic Plaques in Angiographic Manifest Cardiac Allograft Vasculopathy in Long-term Heart Transplanted Patients Using Optical Coherence Tomography
- PMID: 34966839
- PMCID: PMC8710340
- DOI: 10.1097/TXD.0000000000001266
Analysis of Fibrotic Plaques in Angiographic Manifest Cardiac Allograft Vasculopathy in Long-term Heart Transplanted Patients Using Optical Coherence Tomography
Abstract
Background: The development and progression of cardiac allograft vasculopathy documented by coronary angiography (CAVangio) after heart transplantation (HTx) has prognostic relevance. Yet there are limited data regarding the role of concomitant intracoronary imaging in the presence CAVangio. In particular, atherosclerotic plaques might represent a potential target for prevention, but their impact on stenosis is understudied.
Methods: We used high-resolution intracoronary optical coherence tomography (OCT) to quantify and compare findings of intimal hyperplasia (IH) and plaque morphologies in HTx patients (fibrotic plaque, lipid plaque, and calcified plaque). OCT findings were related to the presence of CAVangio as well as to the severity of stenosis.
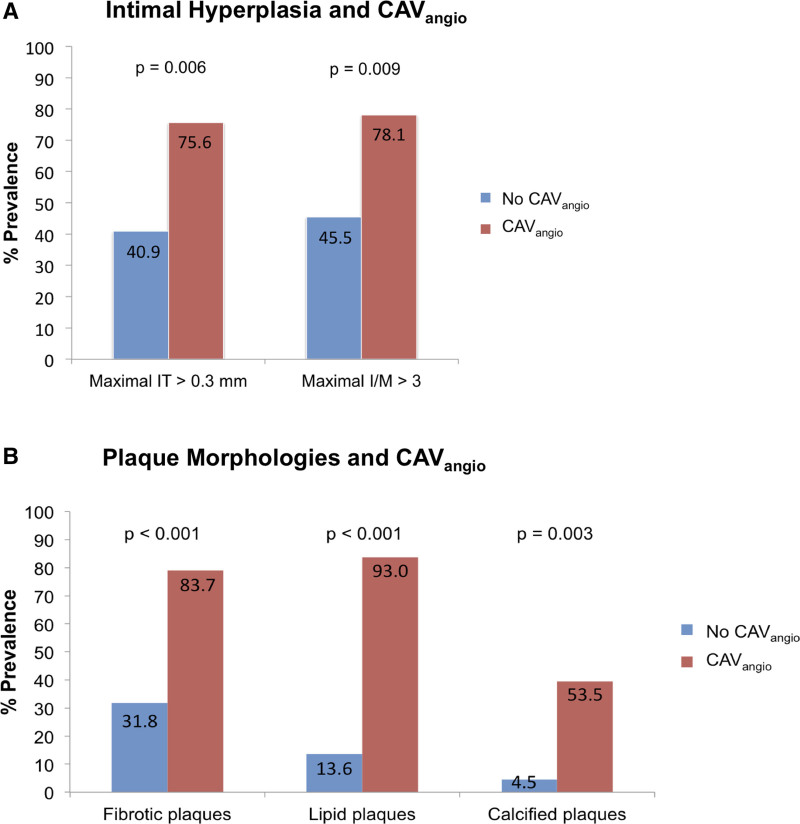
Results: We included 65 consecutive patients into analysis (66% with CAVangio, posttransplant interval 9.9 ± 7.6 y). Fibrotic, lipid, and calcified plaques were present in 41 (63.1%), 39 (60%), and 18 (27.7%) patients, respectively. In addition to IH, the presence of fibrotic, lipid, and calcified plaques was found to be associated with CAVangio. The prevalence of lipid plaque and quantitative measurements of fibrotic plaque increased with stenosis severity (lipid plaque, P < 0.001, maximal and mean fibrotic arc, P = 0.05 and P = 0.001, respectively). Receiver operating characteristic analysis showed that area under the curve of the fibrotic plaque parameter mean fibrotic arc (0.87, 95% confidence interval [0.76-0.99]; P = 0.002) was superior to area under the curve of intima parameters regarding CAVangio. The effect of mean fibrotic arc (r = 0.52, P < 0.001) was relevant regarding stenosis severity.
Conclusions: After a longer posttransplant interval, CAV findings in OCT included a combination of IH and atherosclerotic plaques. In addition to IH, the presence of fibrotic, lipid, and calcified plaques is associated with CAVangio. Further studies are warranted to evaluate if the in vivo screening for plaque progress, particularly of fibrotic plaque, could improve individual secondary prevention and outcome in HTx patients.
Copyright © 2021 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
S.U. reports grants from Novartis Pharma GmbH and Astellas Pharma GmbH, outside the submitted work. M.W.O. received speaker honoraria from Abbott Medical, AstraZeneca, Abiomed, Bayer vital, BIOTRONIK, Bristol Myers Squibb, CytoSorbents, Daiichi Sankyo Deutschland, Edwards Lifesciences Services, Sedana Medical, outside the submitted work. D.B. reports speaker honoraria from Abbott Vascular, outside the submitted work. J.H. reports grants and personal fees from Abbott Vascular, grants and personal fees from Edwards Lifesciences, outside the submitted work. J.M. reports grants and personal fees from Boston Scientifics, Astra Zeneca, Bristol Myers Squibb, Edward Life Science, outside the submitted work. S.M. reports grants from German Federal Ministry of Education and Research (BMBF)/German Centre for Cardiovascular Research (DZHK), grants from German Research Foundation (DFG), grants from Boston scientific, grants from Foundation Leduq Transatlantic Network of Excellence, outside the submitted work. The other authors declare no conflicts of interest.
Figures


References
-
- Chih S, Chong AY, Mielniczuk LM, et al. . Allograft vasculopathy: the Achilles’ heel of heart transplantation. J Am Coll Cardiol. 2016;68:80–91. - PubMed
-
- Mehra MR, Crespo-Leiro MG, Dipchand A, et al. . International Society for Heart and Lung Transplantation working formulation of a standardized nomenclature for cardiac allograft vasculopathy-2010. J Heart Lung Transplant. 2010;29:717–727. - PubMed
-
- Tremblay-Gravel M, Racine N, de Denus S, et al. . Changes in outcomes of cardiac allograft vasculopathy over 30 years following heart transplantation. JACC Heart Fail. 2017;5:891–901. - PubMed
-
- Tsutsui H, Ziada KM, Schoenhagen P, et al. . Lumen loss in transplant coronary artery disease is a biphasic process involving early intimal thickening and late constrictive remodeling: results from a 5-year serial intravascular ultrasound study. Circulation. 2001;104:653–657. - PubMed
LinkOut - more resources
Full Text Sources
