

Inhaled remdesivir reduces viral burden in a nonhuman primate model of SARS-CoV-2 infection
- PMID: 34968150
- PMCID: PMC8961622
- DOI: 10.1126/scitranslmed.abl8282
Inhaled remdesivir reduces viral burden in a nonhuman primate model of SARS-CoV-2 infection
Abstract
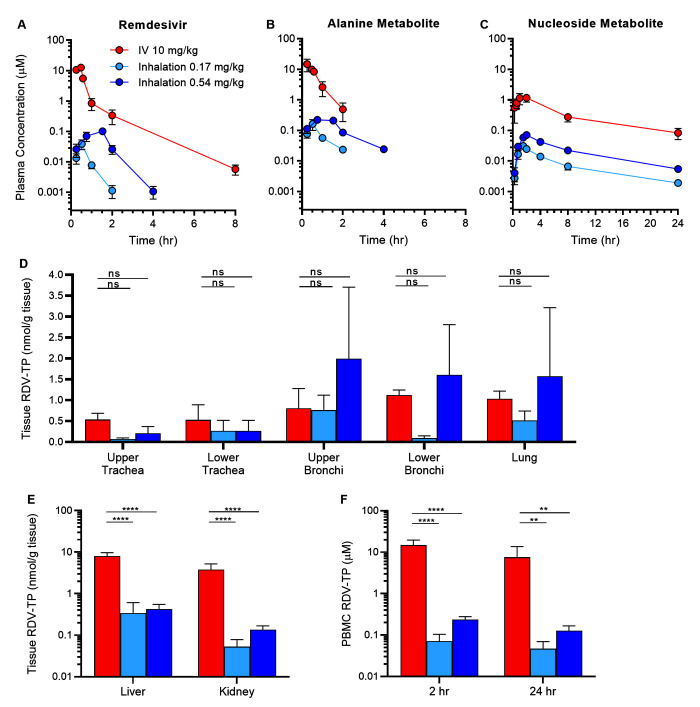
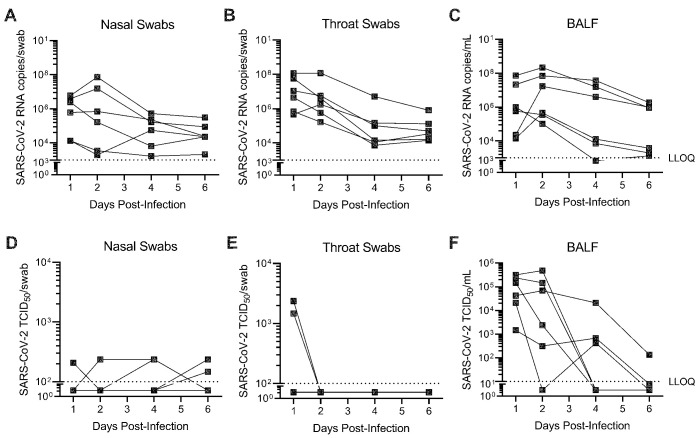
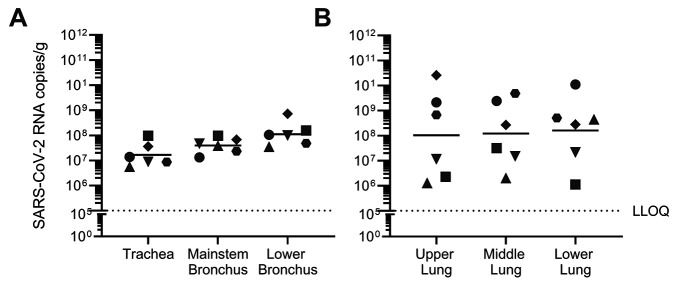
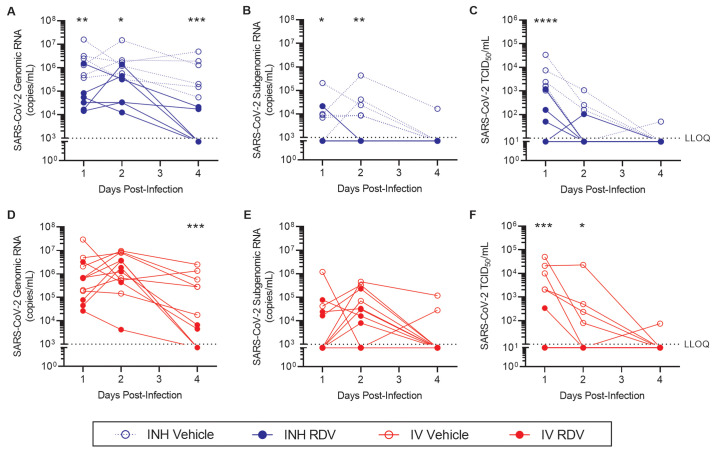
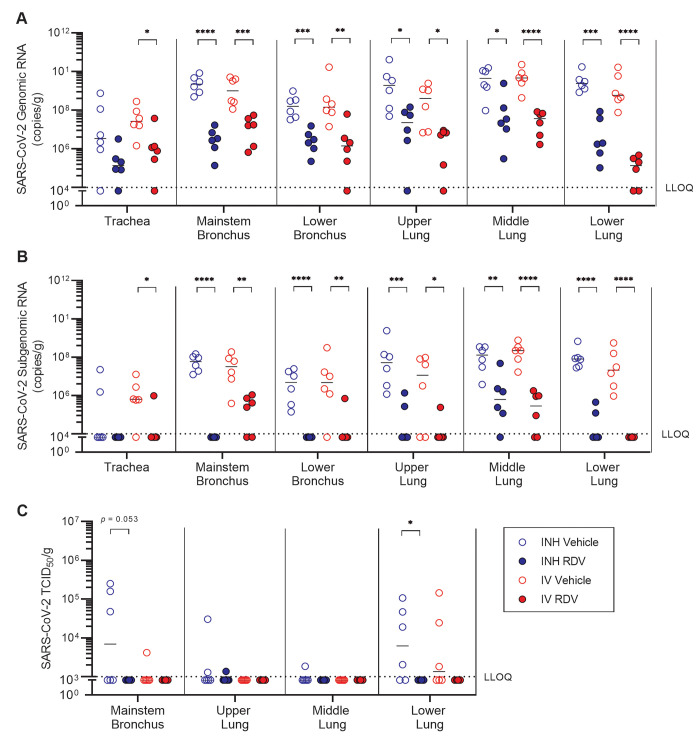
Remdesivir (RDV) is a nucleotide analog prodrug with demonstrated clinical benefit in patients with coronavirus disease 2019 (COVID-19). In October 2020, the US FDA approved intravenous (IV) RDV as the first treatment for hospitalized COVID-19 patients. Furthermore, RDV has been approved or authorized for emergency use in more than 50 countries. To make RDV more convenient for non-hospitalized patients earlier in disease, alternative routes of administration are being evaluated. Here, we investigated the pharmacokinetics and efficacy of RDV administered by head dome inhalation in African green monkeys (AGM). Relative to an IV administration of RDV at 10 mg/kg, an approximately 20-fold lower dose administered by inhalation produced comparable concentrations of the pharmacologically active triphosphate in lower respiratory tract tissues. Distribution of the active triphosphate into the upper respiratory tract was also observed following inhaled RDV exposure. Inhalation RDV dosing resulted in lower systemic exposures to RDV and its metabolites as compared with IV RDV dosing. An efficacy study with repeated dosing of inhaled RDV in an AGM model of SARS-CoV-2 infection demonstrated reductions in viral replication in bronchoalveolar lavage fluid and respiratory tract tissues compared with placebo. Efficacy was observed with inhaled RDV administered once daily at a pulmonary deposited dose of 0.35 mg/kg beginning approximately 8 hours post-infection. Moreover, the efficacy of inhaled RDV was similar to that of IV RDV administered once at 10 mg/kg followed by 5 mg/kg daily in the same study. Together, these findings support further clinical development of inhalation RDV.
Figures
References
-
- Ksiazek T. G., Erdman D., Goldsmith C. S., Zaki S. R., Peret T., Emery S., Tong S., Urbani C., Comer J. A., Lim W., Rollin P. E., Dowell S. F., Ling A.-E., Humphrey C. D., Shieh W.-J., Guarner J., Paddock C. D., Rota P., Fields B., DeRisi J., Yang J.-Y., Cox N., Hughes J. M., LeDuc J. W., Bellini W. J., Anderson L. J.; SARS Working Group , A novel coronavirus associated with severe acute respiratory syndrome. N. Engl. J. Med. 348, 1953–1966 (2003). 10.1056/NEJMoa030781 - DOI - PubMed
-
- Assiri A., Al-Tawfiq J. A., Al-Rabeeah A. A., Al-Rabiah F. A., Al-Hajjar S., Al-Barrak A., Flemban H., Al-Nassir W. N., Balkhy H. H., Al-Hakeem R. F., Makhdoom H. Q., Zumla A. I., Memish Z. A., Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: A descriptive study. Lancet Infect. Dis. 13, 752–761 (2013). 10.1016/S1473-3099(13)70204-4 - DOI - PMC - PubMed
-
- Choi W. S., Kang C. I., Kim Y., Choi J. P., Joh J. S., Shin H. S., Kim G., Peck K. R., Chung D. R., Kim H. O., Song S. H., Kim Y. R., Sohn K. M., Jung Y., Bang J. H., Kim N. J., Lee K. S., Jeong H. W., Rhee J.-Y., Kim E. S., Woo H., Oh W. S., Huh K., Lee Y. H., Song J. Y., Lee J., Lee C.-S., Kim B.-N., Choi Y. H., Jeong S. J., Lee J.-S., Yoon J. H., Wi Y. M., Joung M. K., Park S. Y., Lee S. H., Jung S.-I., Kim S.-W., Lee J. H., Lee H., Ki H. K., Kim Y.-S.; Korean Society of Infectious Diseases , Clinical Presentation and Outcomes of Middle East Respiratory Syndrome in the Republic of Korea. Infect. Chemother. 48, 118–126 (2016). 10.3947/ic.2016.48.2.118 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
