

Is comprehensive geriatric assessment hospital at home a cost-effective alternative to hospital admission for older people?
- PMID: 34969074
- PMCID: PMC8753046
- DOI: 10.1093/ageing/afab220
Is comprehensive geriatric assessment hospital at home a cost-effective alternative to hospital admission for older people?
Abstract
Background: hospital level healthcare in the home guided by comprehensive geriatric assessment (CGA) might provide a less costly alternative to hospitalisation for older people.
Objective: to determine the cost-effectiveness of CGA admission avoidance hospital at home (HAH) compared with hospital admission.
Design/intervention: a cost-effectiveness study alongside a randomised trial of CGA in an admission avoidance HAH setting, compared with admission to hospital.
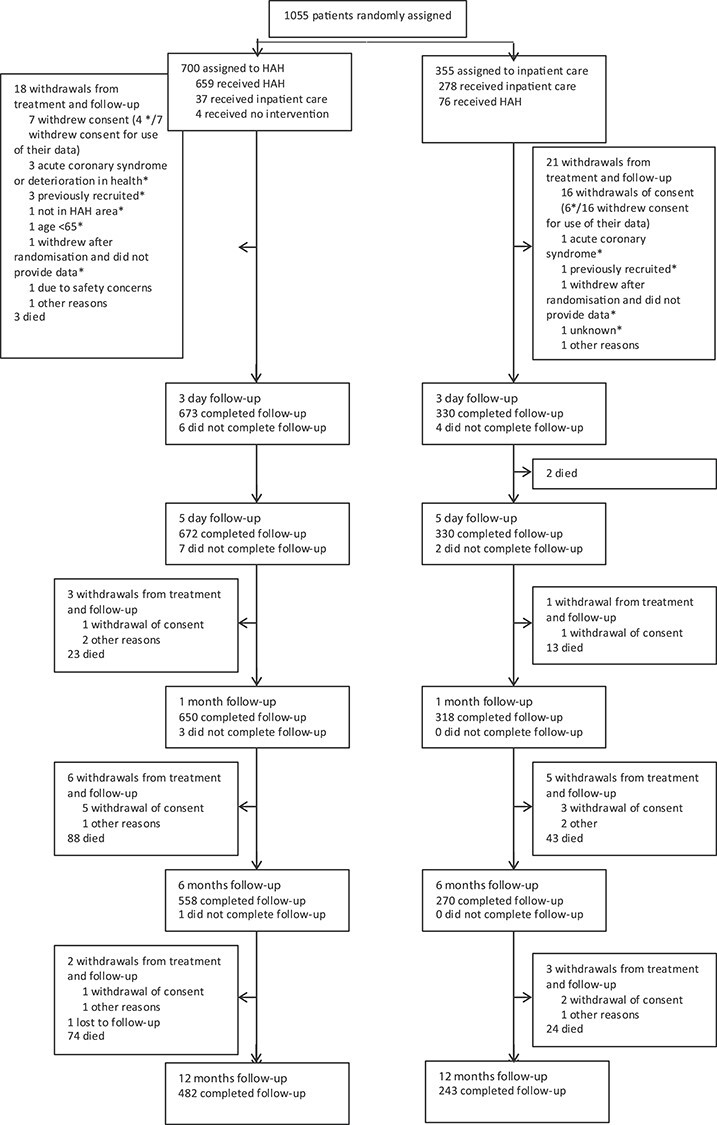
Participants/setting: older people considered for a hospital admission in nine locations across the UK were randomised using a 2:1 randomisation schedule to admission avoidance HAH with CGA (N = 700), or admission to hospital with CGA when available (N = 355).
Measurements: quality adjusted life years, resource use and costs at baseline and 6 months; incremental cost-effectiveness ratios were calculated. The main analysis used complete cases.
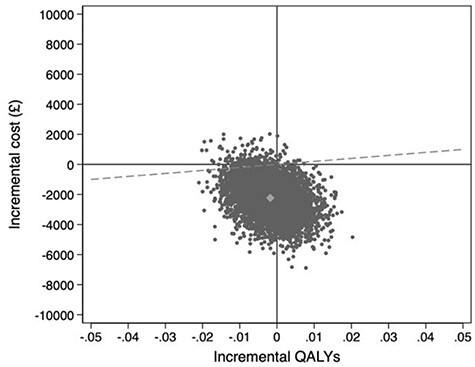
Results: adjusting for baseline covariates, HAH was less costly than admission to hospital from a health and social care perspective (mean -£2,265, 95% CI: -4,279 to -252), and remained less costly with the addition of informal care costs (mean difference -£2,840, 95% CI: -5,495 to -185). There was no difference in quality adjusted survival. Using multiple imputation for missing data, the mean difference in health and social care costs widened to -£2,458 (95% CI: -4,977 to 61) and societal costs remained significantly lower (-£3,083, 95% CI: -5,880 to -287). There was little change to quality adjusted survival.
Conclusions: CGA HAH is a cost-effective alternative to admission to hospital for selected older people.
Keywords: admission avoidance hospital at home; comprehensive geriatric assessment; cost-effectiveness; older people.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Geriatrics Society. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Prince MJ, Wu F, Guo Y et al. The burden of disease in older people and implications for health policy and practice. Lancet 2015; 385: 549–62. - PubMed
-
- Department of Health & Social Care NHS England . Reducing Emergency Admissions. London: National Audit Office. 2018. https://www.nao.org.uk/wp-content/uploads/2018/02/Reducing-emergency-adm... (6 April 2021, date last accessed.
-
- OECD . Fiscal Sustainability of Health Systems: Bridging Health and Finance Perspectives. OECD Publising; Paris; 2015. 10.1787/9789264233386-en (6 April 2021, date last accessed). - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
