

Phase 2 trial design of BMS-986278, a lysophosphatidic acid receptor 1 (LPA1) antagonist, in patients with idiopathic pulmonary fibrosis (IPF) or progressive fibrotic interstitial lung disease (PF-ILD)
- PMID: 34969771
- PMCID: PMC8718498
- DOI: 10.1136/bmjresp-2021-001026
Phase 2 trial design of BMS-986278, a lysophosphatidic acid receptor 1 (LPA1) antagonist, in patients with idiopathic pulmonary fibrosis (IPF) or progressive fibrotic interstitial lung disease (PF-ILD)
Abstract
Introduction: Idiopathic pulmonary fibrosis (IPF) and non-IPF, progressive fibrotic interstitial lung diseases (PF-ILD), are associated with a progressive loss of lung function and a poor prognosis. Treatment with antifibrotic agents can slow, but not halt, disease progression, and treatment discontinuation because of adverse events is common. Fibrotic diseases such as these can be mediated by lysophosphatidic acid (LPA), which signals via six LPA receptors (LPA1-6). Signalling via LPA1 appears to be fundamental in the pathogenesis of fibrotic diseases. BMS-986278, a second-generation LPA1 antagonist, is currently in phase 2 development as a therapy for IPF and PF-ILD.
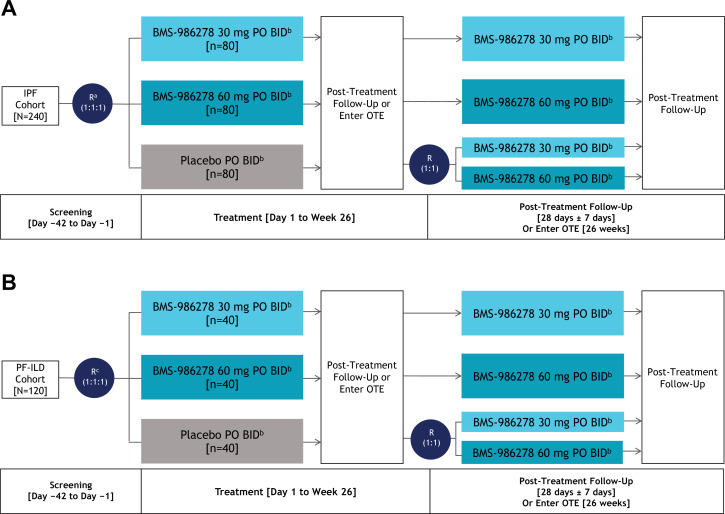
Methods and analysis: This phase 2, randomised, double-blind, placebo-controlled, parallel-group, international trial will include adults with IPF or PF-ILD. The trial will consist of a 42-day screening period, a 26-week placebo-controlled treatment period, an optional 26-week active-treatment extension period, and a 28-day post-treatment follow-up. Patients in both the IPF (n=240) and PF-ILD (n=120) cohorts will be randomised 1:1:1 to receive 30 mg or 60 mg BMS-986278, or placebo, administered orally two times per day for 26 weeks in the placebo-controlled treatment period. The primary endpoint is rate of change in per cent predicted forced vital capacity from baseline to week 26 in the IPF cohort.
Ethics and dissemination: This study will be conducted in accordance with Good Clinical Practice guidelines, Declaration of Helsinki principles, and local ethical and legal requirements. Results will be reported in a peer-reviewed publication.
Trial registration number: NCT04308681.
Keywords: interstitial fibrosis.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: TJC has served on advisory boards for Boehringer Ingelheim, Hoffman-LaRoche, Bristol Myers Squibb, Ad-Alta, Promedior and Prometic Life Sciences. Her institution has received grants or research fees from Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Galápagos and Hoffman-La Roche, outside the submitted work. LL has served on advisory boards for United Therapeutics, Bristol Myers Squibb, AstraZeneca, Galápagos, Genentech and DevPro Biopharma; and has received research funding from Biogen, Celgene, Novartis, Bellerophon Therapeutics, Galecto, Bristol Myers Squibb, Respivant Sciences, Galápagos, Boehringer Ingelheim, Roche and Pliant Therapeutics; and has provided disease-state education for Genentech, Boehringer Ingelheim, United Therapeutics and Veracyte. JJS receives honoraria from Genentech for giving unbranded, disease-state talks on IPF; he also receives grant support from Genentech and Boehringer Ingelheim. He is a paid consultant for Boehringer Ingelheim and an unpaid consultant for Bristol Myers Squibb. TMM has received personal fees from AstraZeneca, Bayer, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Galápagos, GlaxoSmithKline, Indalo Therapeutics, Pliant Therapeutics, Roche, and UCB, outside the submitted work. His institution received grants or research fees from AstraZeneca, GlaxoSmithKline and UCB outside the submitted work. JGG is the founder of MedQIA, LLC. SMP has consulted or served on advisory boards for Boehringer Ingelheim, Bristol Myers Squibb and Altavant; and has received research funding to Duke from Boehringer Ingelheim, Bristol Myers Squibb and AstraZeneca. TS has served on advisory boards for Bristol Myers Squibb and has received an honorarium and research funding from Boehringer Ingelheim. TO has served on advisory boards for Bristol Myers Squibb and has received personal fees from Boehringer Ingelheim, Shionogi, Astellas Pharma and Toray industries. AM is a consultant for Bristol Myers Squibb. XZ, GST, BE, HX, HW, RAS, EDC and AF are all employees of Bristol Myers Squibb.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous