

Treatment of Cryptogenic Stroke Patients with Atrial Fibrillation Detected by Insertable Cardiac Monitors Reduces Recurrent Stroke Risk to Background Levels
- PMID: 34970471
- PMCID: PMC8711968
- DOI: 10.19102/icrm.2021.121204
Treatment of Cryptogenic Stroke Patients with Atrial Fibrillation Detected by Insertable Cardiac Monitors Reduces Recurrent Stroke Risk to Background Levels
Abstract
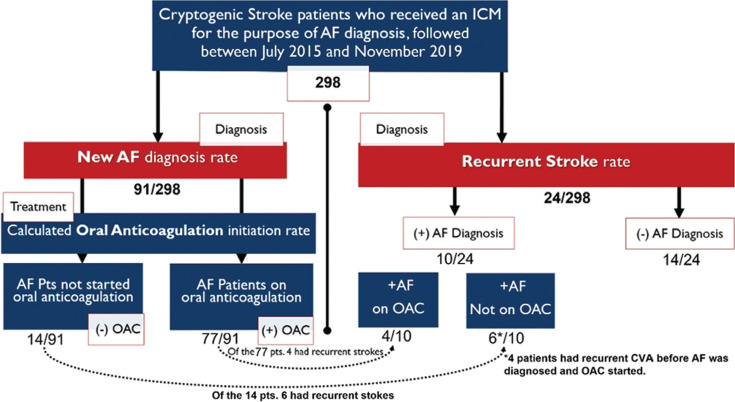
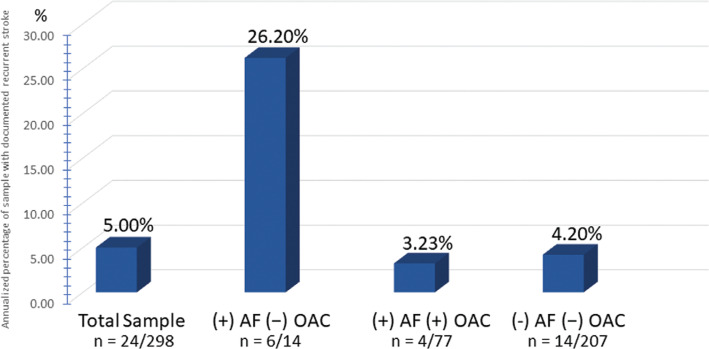
Atrial fibrillation (AF) is a known risk factor of ischemic stroke with a reported fivefold increase in incidence. However, it is not well established whether treatment with oral anticoagulation (OAC) in cryptogenic stroke patients with AF, detected by insertable cardiac monitors (ICMs), reduces the risk of recurrent stroke. We aimed to compare recurrent stroke rates between cryptogenic stroke patients who have AF detected by ICMs and thus started on OAC treatment and those without detected AF. We performed a combined retrospective and prospective analysis of consecutive patients who received an ICM indicated for cryptogenic stroke and were followed up with between July 2015 and November 2019. Patients with a prior documented history of AF were excluded. All patients were required to have a home remote monitoring system. We calculated the rates of AF detection and OAC initiation, then compared recurrent annualized stroke rates (ASRs) between patients with and without AF detected. A total of 298 patients with ICMs were included in the study [mean ± standard deviation age: 77 ± 11.7 years; female/male: 147/151; virtual CHA2DS2-VASc score: 4.96 ± 1.28 points]. AF was discovered in 91 patients (~30%) over a mean 19.3 months follow-up. Of those, 65 (71.4%) were started on OAC, 12 (13.2%) were already on OAC, and 10 (11%) remained non-anticoagulated. In four (4.4%) patients, OAC was started after recurrent stroke when AF was diagnosed. A total of 24 of 298 patients developed recurrent strokes (ASR: 5.0%). Among the 24 patients with recurrent strokes, four had new AF and were on OAC (ASR: 3.23%), six had new AF and were not anticoagulated (ASR: 26.62%), and 14 had no AF detected and no OAC (ASR: 4.20%). Our study found new AF detected by ICMs in almost one-third (30%) of cryptogenic stroke patients (consistent with previous studies), and the majority of them (89%) received OACs. There was no significant difference in the recurrent stroke rate among patients without AF detected and those with AF detected and on OAC. Rigorous arrhythmia monitoring using ICMs can increase new AF detection rates in cryptogenic stroke patients, thereby allowing early initiation of OACs, ultimately reducing the risk of recurrent stroke to background levels.
Keywords: Atrial fibrillation; cryptogenic stroke; guided oral anticoagulation therapy; implantable cardiac monitor; stroke reduction.
Copyright: © 2021 Innovations in Cardiac Rhythm Management.
Conflict of interest statement
Dr. Kloosterman receives a modest honorary from Medtronic for research support (not related to this study) and serves as a consultant and a speaker. The other authors report no conflicts of interest for the published content.
Figures
References
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham study. Stroke. 1991;22(8):983–988. [CrossRef] [PubMed] - DOI - PubMed
-
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480. [CrossRef] [PubMed] - DOI - PMC - PubMed
-
- Virani SS, Alonso A, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2020 Update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596. [CrossRef] [PubMed] - DOI - PubMed
-
- Li L, Yiin GS, Geraghty OC, et al. Incidence, outcome, risk factors, and long-term prognosis of cryptogenic transient ischemic attack and ischemic stroke: a population-based study. Lancet Neurol. 2015;14(9):903–913. [CrossRef] [PubMed] - DOI - PMC - PubMed
-
- Brambatti M, Connolly SJ, Gold MR, et al. Temporal relationship between subclinical atrial fibrillation and embolic events. Circulation. 2014;129(21):2094–2099. [CrossRef] [PubMed] - DOI - PubMed
LinkOut - more resources
Full Text Sources