

Reducing complication rates for repeat craniotomies in glioma patients: a single-surgeon experience and comparison with the literature
- PMID: 34970702
- PMCID: PMC8854329
- DOI: 10.1007/s00701-021-05067-9
Reducing complication rates for repeat craniotomies in glioma patients: a single-surgeon experience and comparison with the literature
Abstract
Background: There is a concern that glioma patients undergoing repeat craniotomies are more prone to complications. The study's goal was to assess if the complication profiles for initial and repeat craniotomies were similar, to determine predictors of complications, and to compare results with those in the literature.
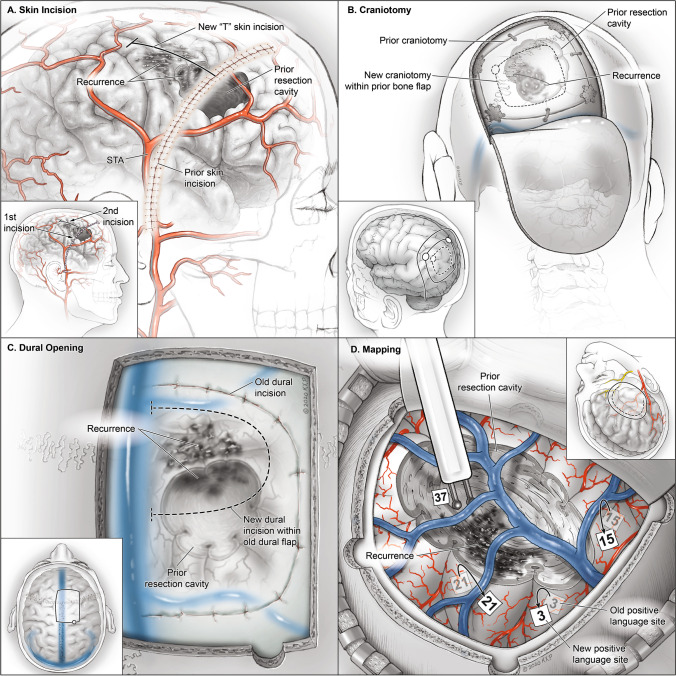
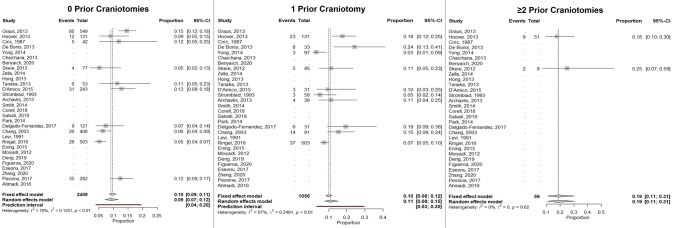
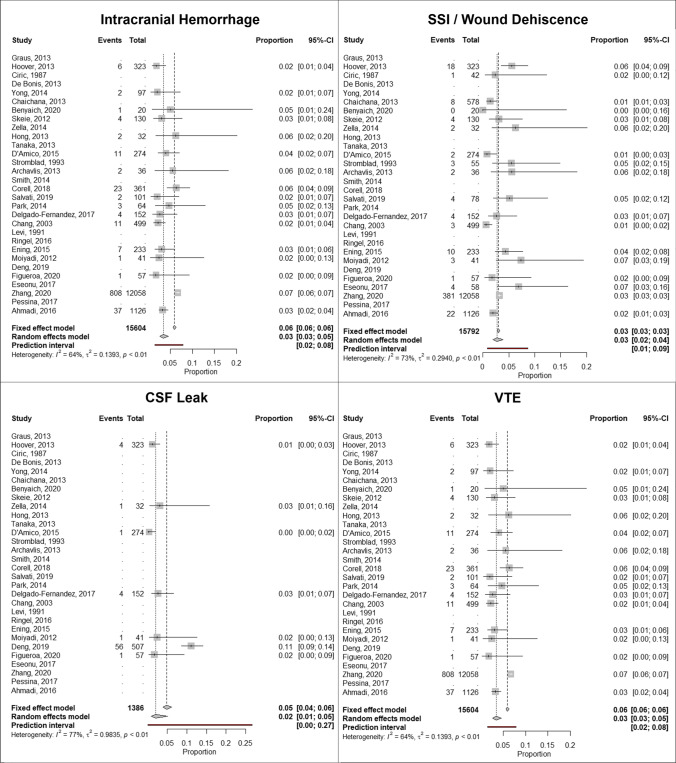
Methods: A retrospective study was conducted of glioma patients (WHO grade II-IV) who underwent either an initial or repeat craniotomy performed by the senior author from 2012 until 2019. Complications were recorded by discharge, 30 days, and 90 days postoperatively. New neurologic deficits were recorded by 90 days postoperatively. Multivariate regression was performed to identify factors associated with complications. A meta-analysis was performed to identify rates of complications based on number of prior craniotomies.
Results: Within the cohort of 714 patients, 400 (56%) had no prior craniotomies, 218 (30.5%) had undergone 1 prior craniotomy, and 96 (13.5%) had undergone ≥ 2 prior craniotomies. There were 27 surgical and 10 medical complications in 30 patients (4.2%) and 19 reoperations for complications in 19 patients (2.7%) with no deaths by 90 days. Complications, reoperation rates, and new neurologic deficits did not differ based on number of prior craniotomies. On multivariate analysis, older age (OR1.5, 95%CI 1.0-2.2) and significant leukocytosis due to steroid use (OR12.6, 95%CI 2.5-62.9) were predictors of complications. Complication rates in the cohort were lower than rates reported in the literature.
Conclusion: Contrary to prior reports in the literature, repeat craniotomies can be as safe as initial operations if surgeons implement best practices.
Keywords: Complications; Glioma; Recurrence; Surgical resection.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ahmadi R, Campos B, Haux D, Rieke J, Beigel B, Unterberg A. Assessing perioperative complications associated with use of intraoperative magnetic resonance imaging during glioma surgery-a single centre experience with 516 cases. Br J Neurosurg. 2016;30(4):397–400. - PubMed
-
- Barker FG, 2nd, Chang SM, Gutin PH, Malec MK, McDermott MW, Prados MD, Wilson CB. Survival and functional status after resection of recurrent glioblastoma multiforme. Neurosurgery. 1998;42(4):703–709. - PubMed
-
- Benyaich Z, Hajhouji F, Laghmari M, Ghannane H, Aniba K, Lmejjati M, Ait Benali S. Awake craniotomy with functional mapping for glioma resection in a limited-resource-setting: preliminary experience from a lower-middle income country. World neurosurgery. 2020;139:200–207. - PubMed
-
- Bloch O, Han SJ, Cha S, Sun MZ, Aghi MK, McDermott MW, Berger MS, Parsa AT. Impact of extent of resection for recurrent glioblastoma on overall survival: clinical article. J Neurosurg. 2012;117(6):1032–1038. - PubMed
