

GPC2-CAR T cells tuned for low antigen density mediate potent activity against neuroblastoma without toxicity
- PMID: 34971569
- PMCID: PMC9092726
- DOI: 10.1016/j.ccell.2021.12.005
GPC2-CAR T cells tuned for low antigen density mediate potent activity against neuroblastoma without toxicity
Abstract
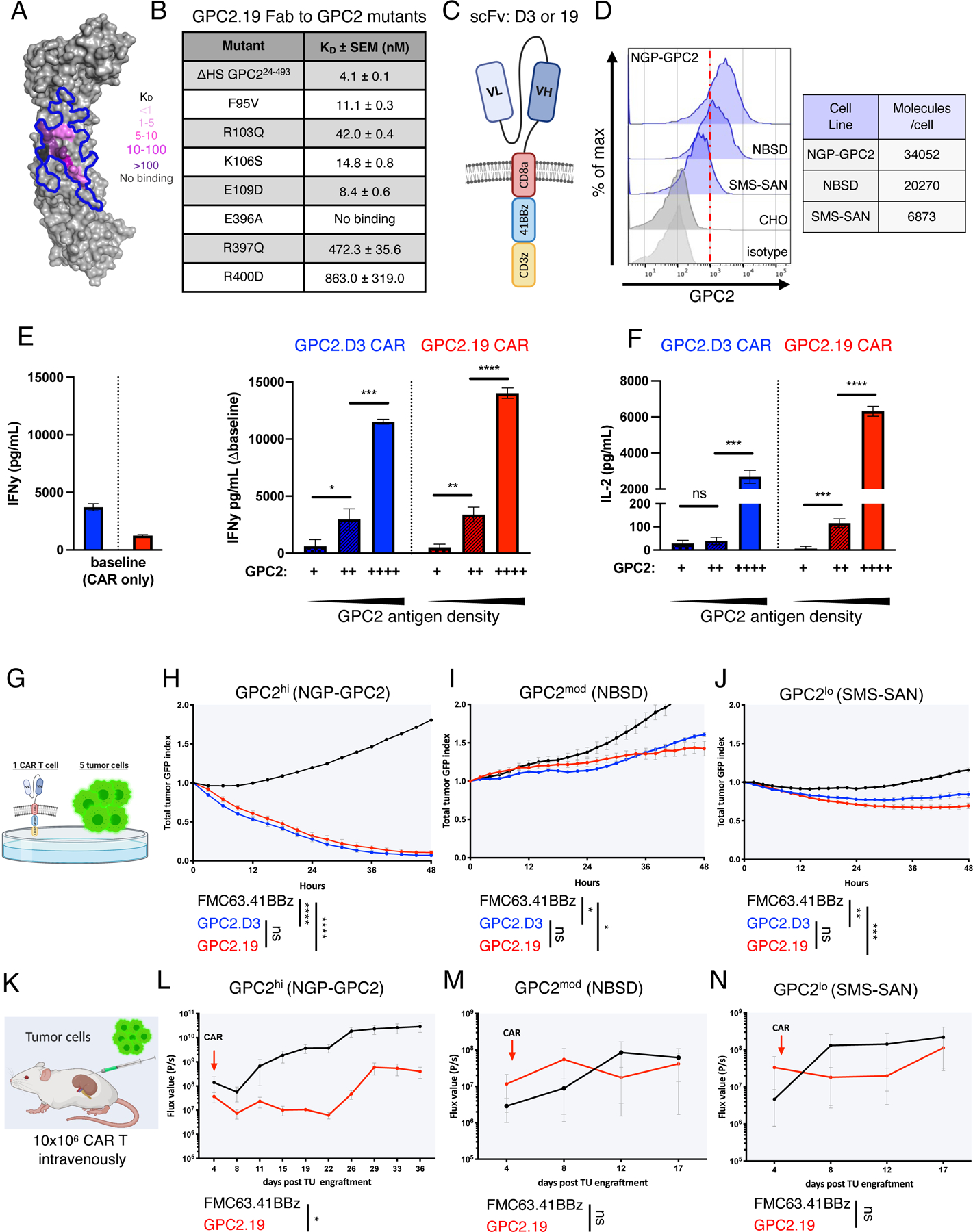
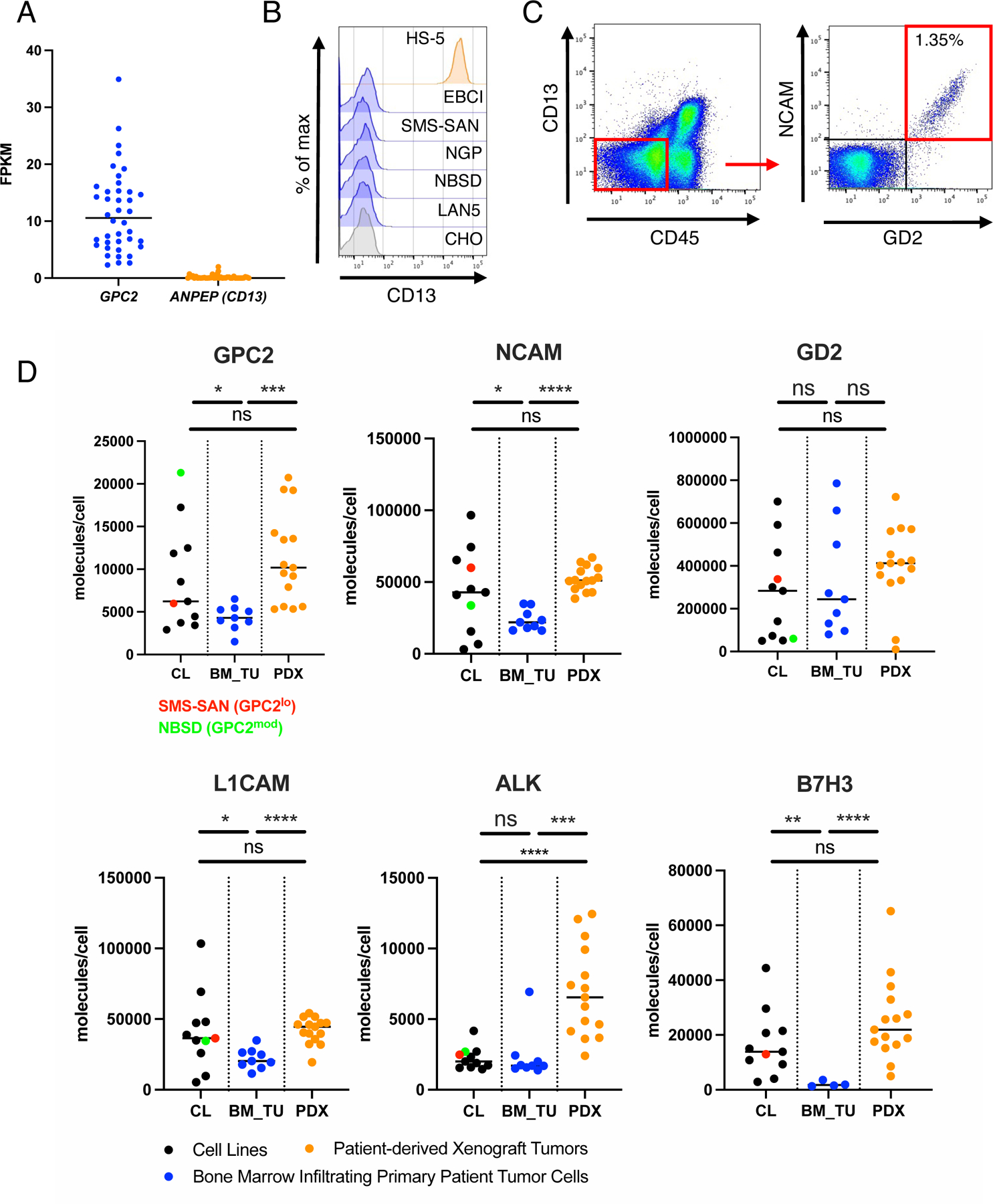
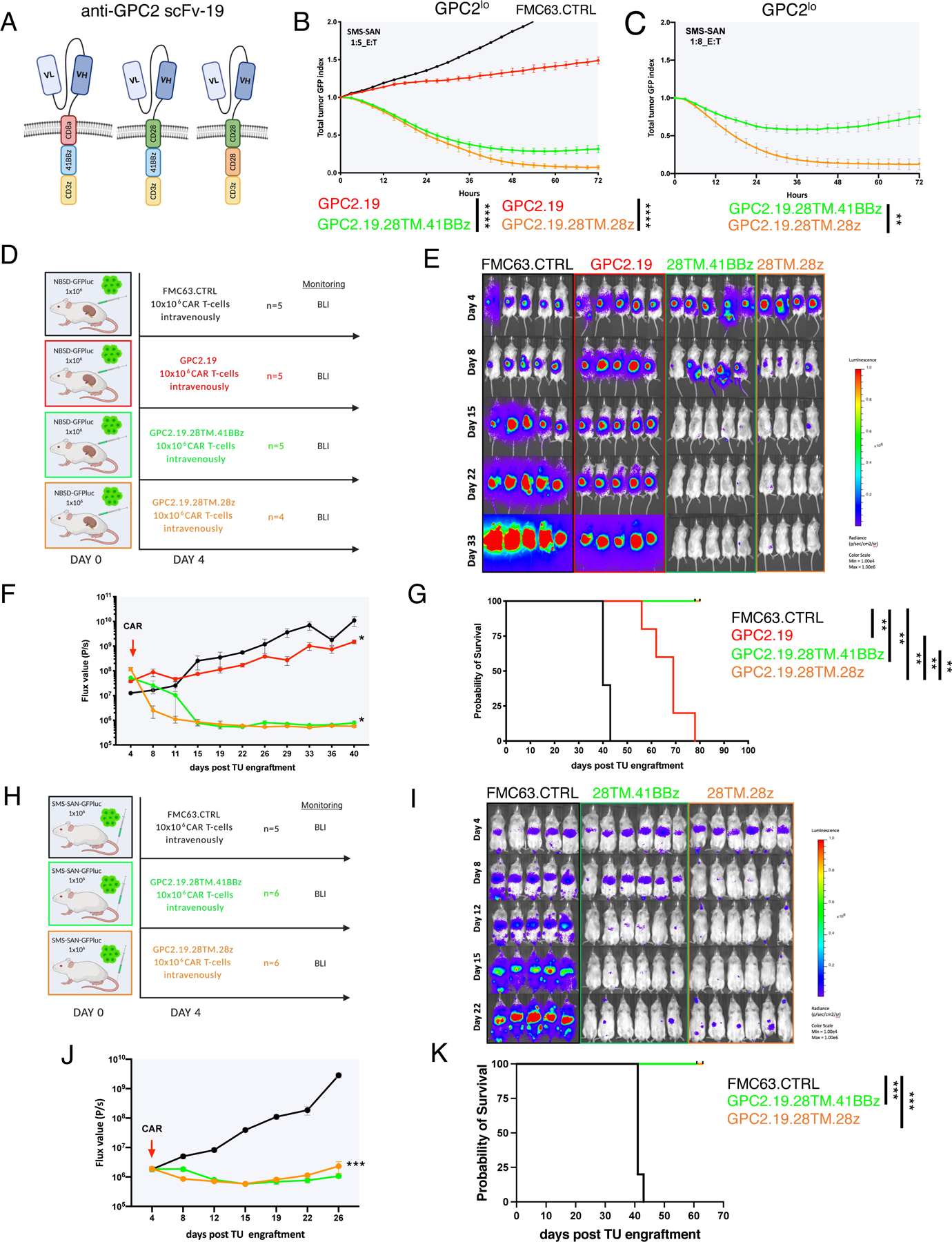
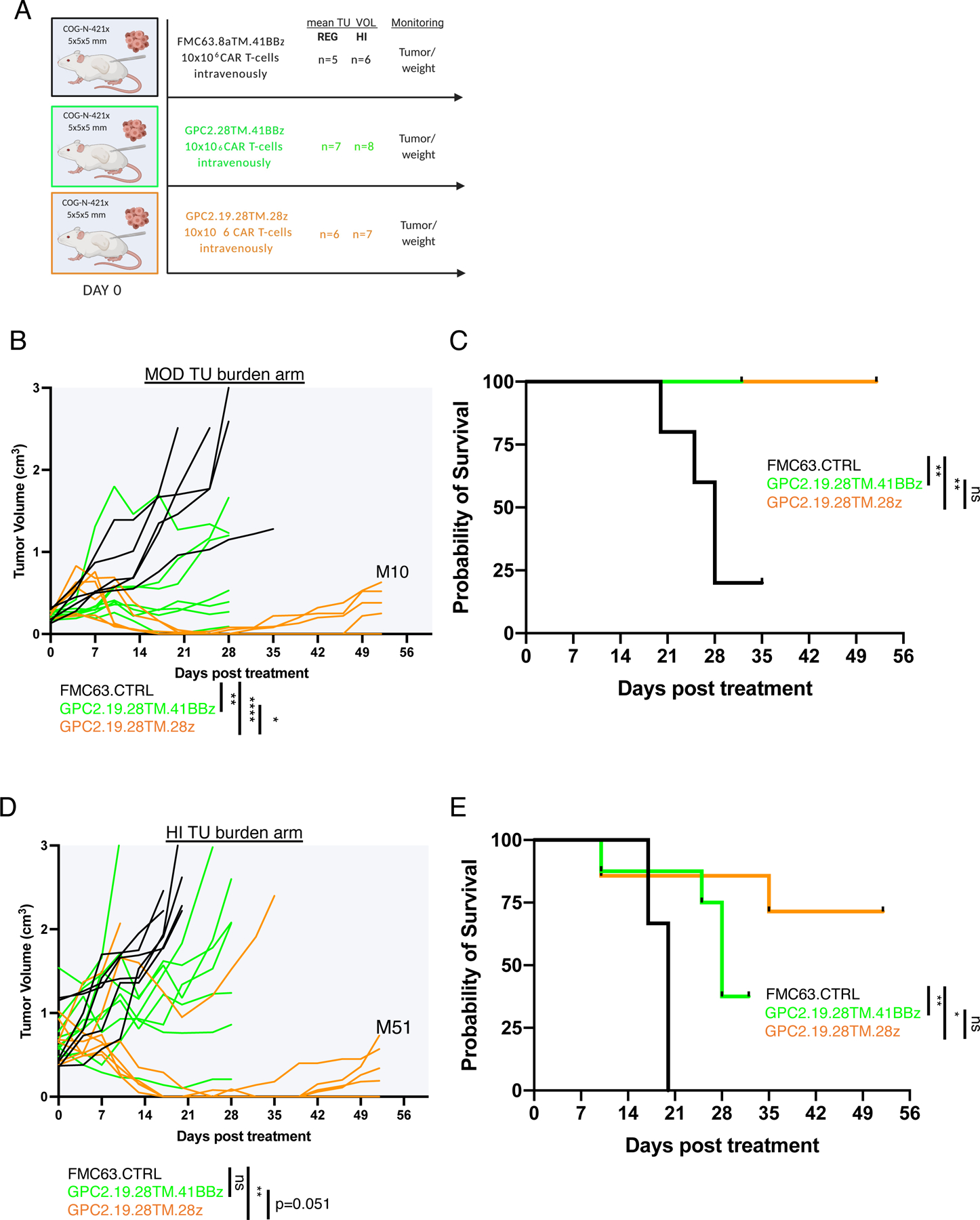
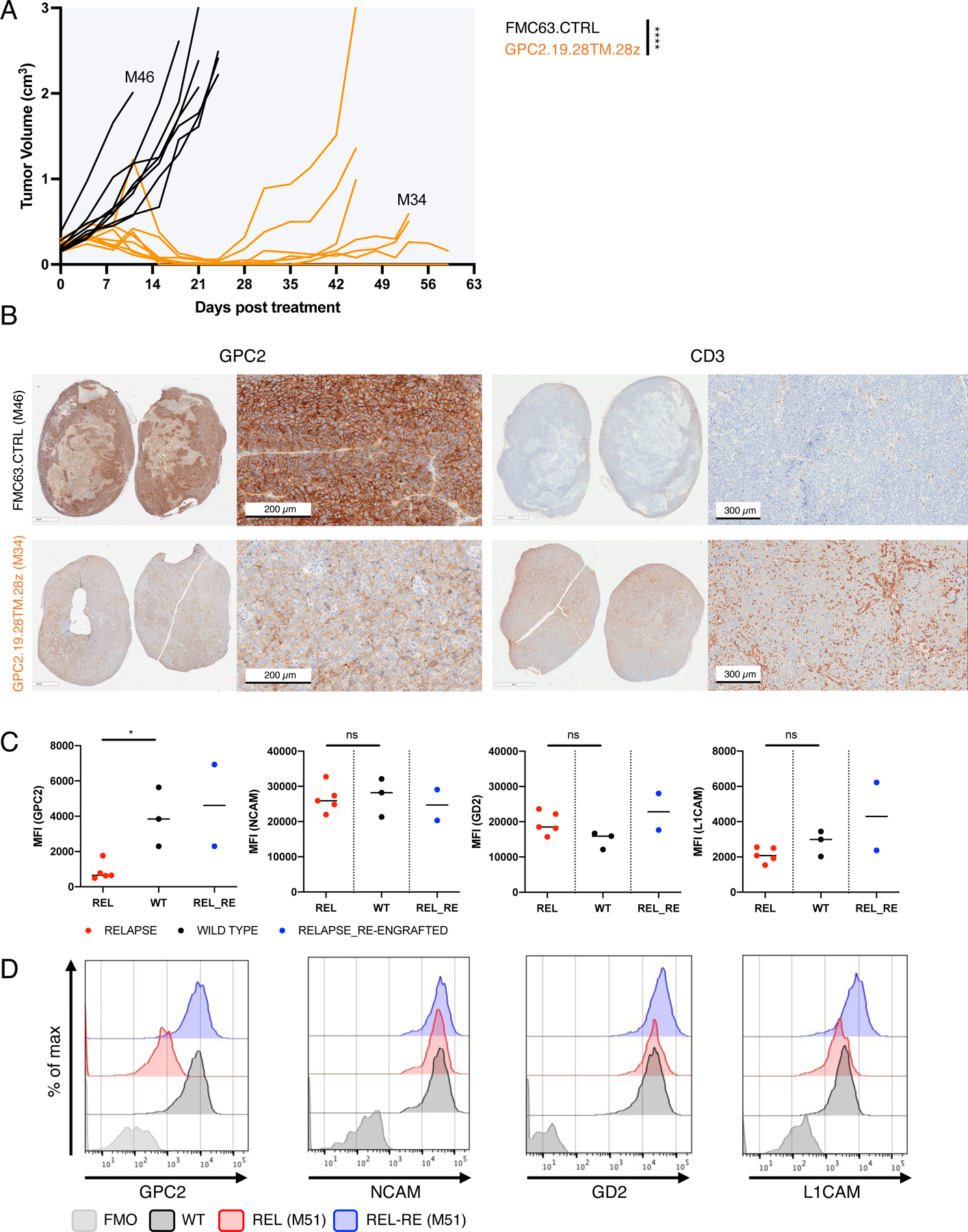
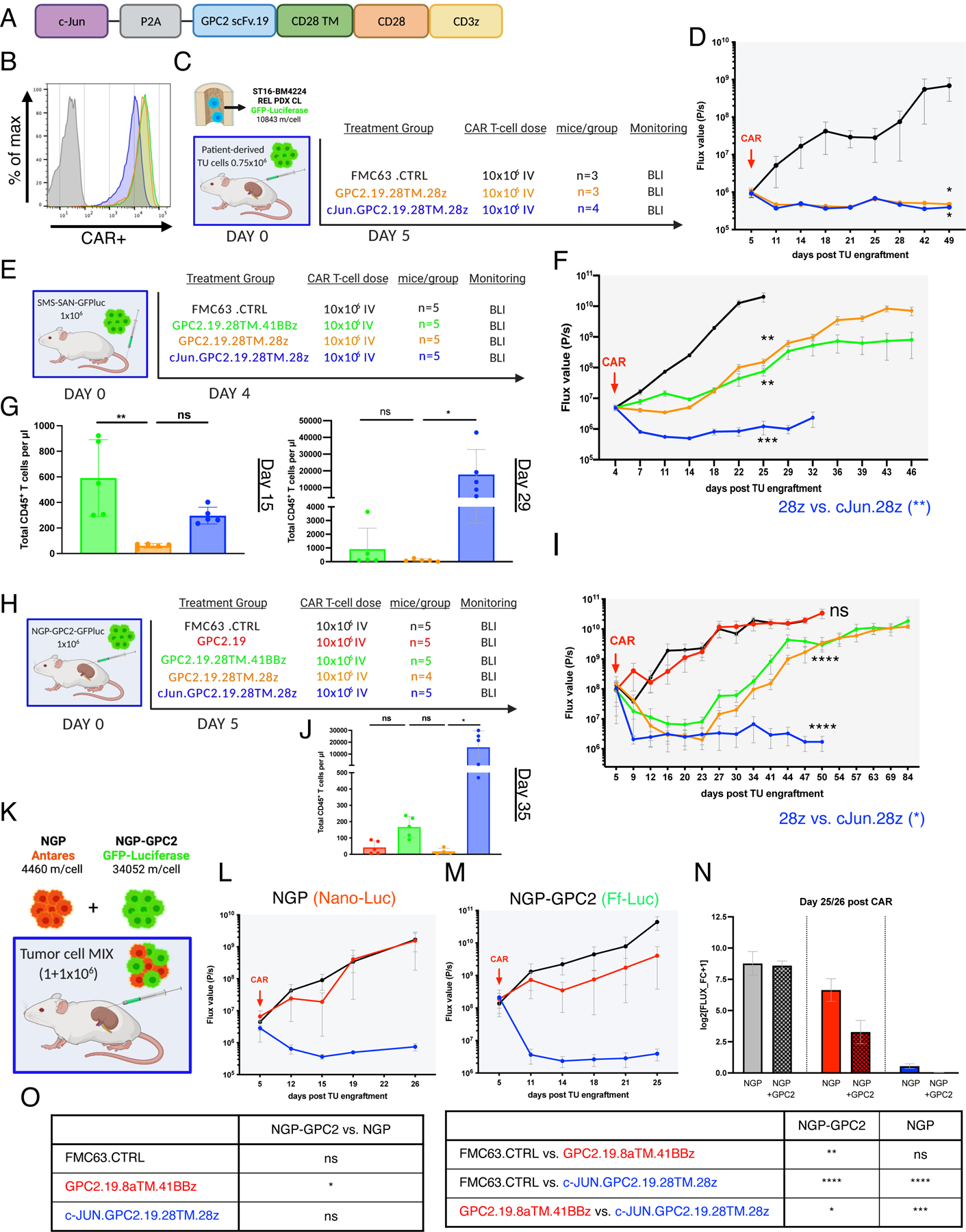
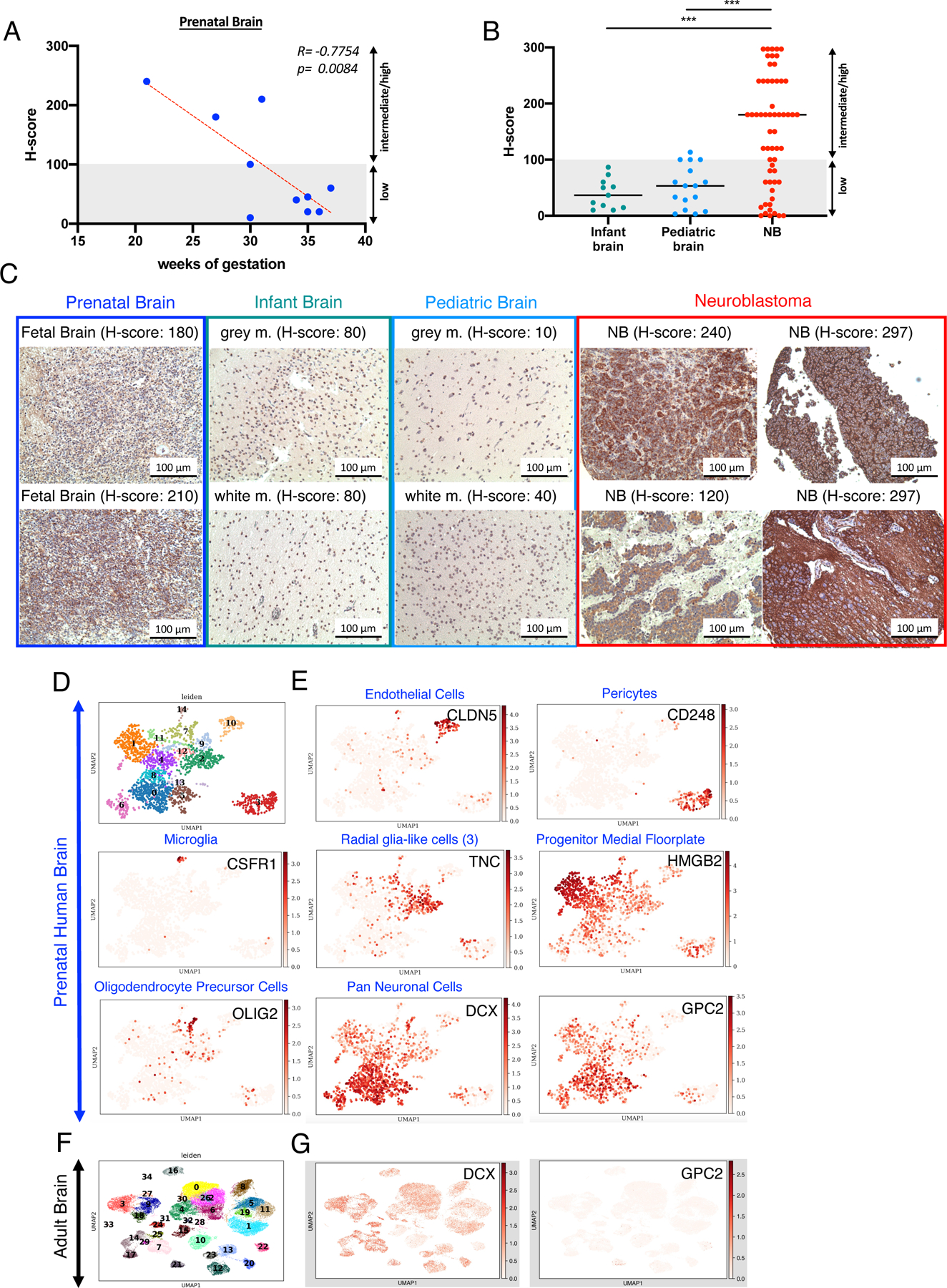
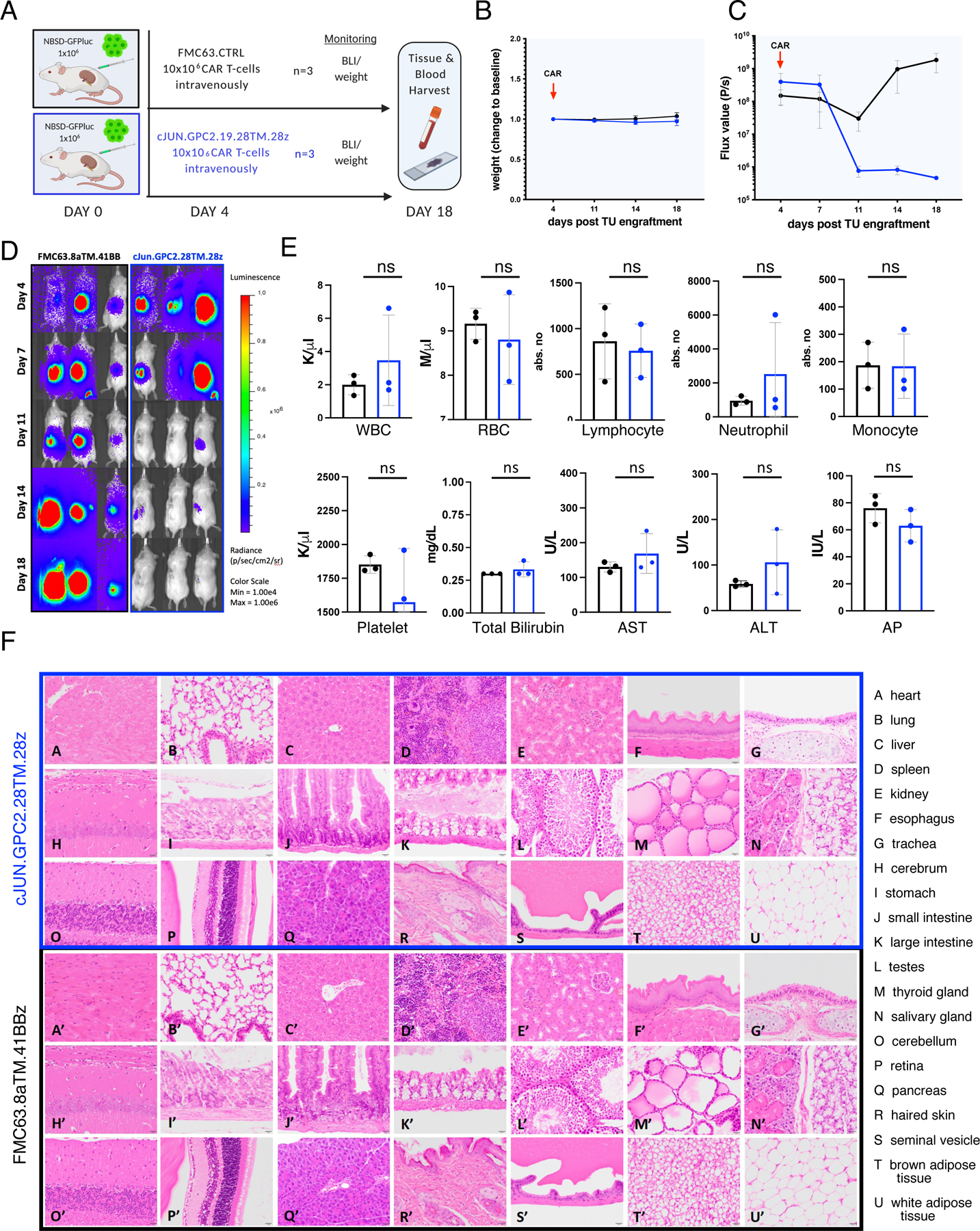
Pediatric cancers often mimic fetal tissues and express proteins normally silenced postnatally that could serve as immune targets. We developed T cells expressing chimeric antigen receptors (CARs) targeting glypican-2 (GPC2), a fetal antigen expressed on neuroblastoma (NB) and several other solid tumors. CARs engineered using standard designs control NBs with transgenic GPC2 overexpression, but not those expressing clinically relevant GPC2 site density (∼5,000 molecules/cell, range 1-6 × 103). Iterative engineering of transmembrane (TM) and co-stimulatory domains plus overexpression of c-Jun lowered the GPC2-CAR antigen density threshold, enabling potent and durable eradication of NBs expressing clinically relevant GPC2 antigen density, without toxicity. These studies highlight the critical interplay between CAR design and antigen density threshold, demonstrate potent efficacy and safety of a lead GPC2-CAR candidate suitable for clinical testing, and credential oncofetal antigens as a promising class of targets for CAR T cell therapy of solid tumors.
Keywords: CAR T cell; GPC2; antigen density; chimeric antigen receptor; glypican-2; immunotherapy; neuroblastoma; oncofetal antigen.
Copyright © 2021. Published by Elsevier Inc.
Conflict of interest statement
Declaration of interest C.L.M., S.H., J.M.M., K.R.B., R.G.M., D.S.D., and Z.Z. are co-inventors on patents related to this work. C.L.M. (and others) have multiple patents pertinent to CAR T cells. C.L.M. is a co-founder of Lyell Immunopharma and Syncopation Life Sciences, which develop CAR-based therapies, and consults for Lyell, NeoImmune Tech, Apricity, Nektar, and Immatics. K.R.B. and J.M.M. receive research funding from Tmunity for research on GPC2-directed immunotherapies. D.Z., Z.Z., D.S.D., J.M.M., and K.R.B. receive royalties from Tmunity for licensing of GPC2-related IP. R.G.M. and E.S. are consultants for and hold equity in Lyell Immunopharma. R.G.M. consults for GammaDelta Therapeutics, Aptorum Group, Zai Lab, and Illumina Radiopharmaceuticals and J.T. for Dorian Therapeutics. S.J.B. is an employee of BD Biosciences. A.T.S. is a founder of Immunai and Cartography Biosciences and receives research funding from Arsenal Biosciences and 10× Genomics. K.R.P. is a co-founder and employee of Cartography Biosciences. H.Y.C. is a co-founder of Accent Therapeutics and Boundless Bio and is an advisor to 10× Genomics, Arsenal Bio, and Spring Discovery.
Figures
Comment in
-
Fine-tuning CARs for best performance.Cancer Cell. 2022 Jan 10;40(1):11-13. doi: 10.1016/j.ccell.2021.12.010. Cancer Cell. 2022. PMID: 35016025
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
