

Hydroxyurea for primary stroke prevention in children with sickle cell anaemia in Nigeria (SPRING): a double-blind, multicentre, randomised, phase 3 trial
- PMID: 34971579
- PMCID: PMC10072240
- DOI: 10.1016/S2352-3026(21)00368-9
Hydroxyurea for primary stroke prevention in children with sickle cell anaemia in Nigeria (SPRING): a double-blind, multicentre, randomised, phase 3 trial
Abstract
Background: In high-income countries, standard care for primary stroke prevention in children with sickle cell anaemia and abnormal transcranial Doppler velocities results in a 92% relative risk reduction of strokes but mandates initial monthly blood transfusion. In Africa, where regular blood transfusion is not feasible for most children, we tested the hypothesis that initial moderate-dose compared with low-dose hydroxyurea decreases the incidence of strokes for children with abnormal transcranial Doppler velocities.
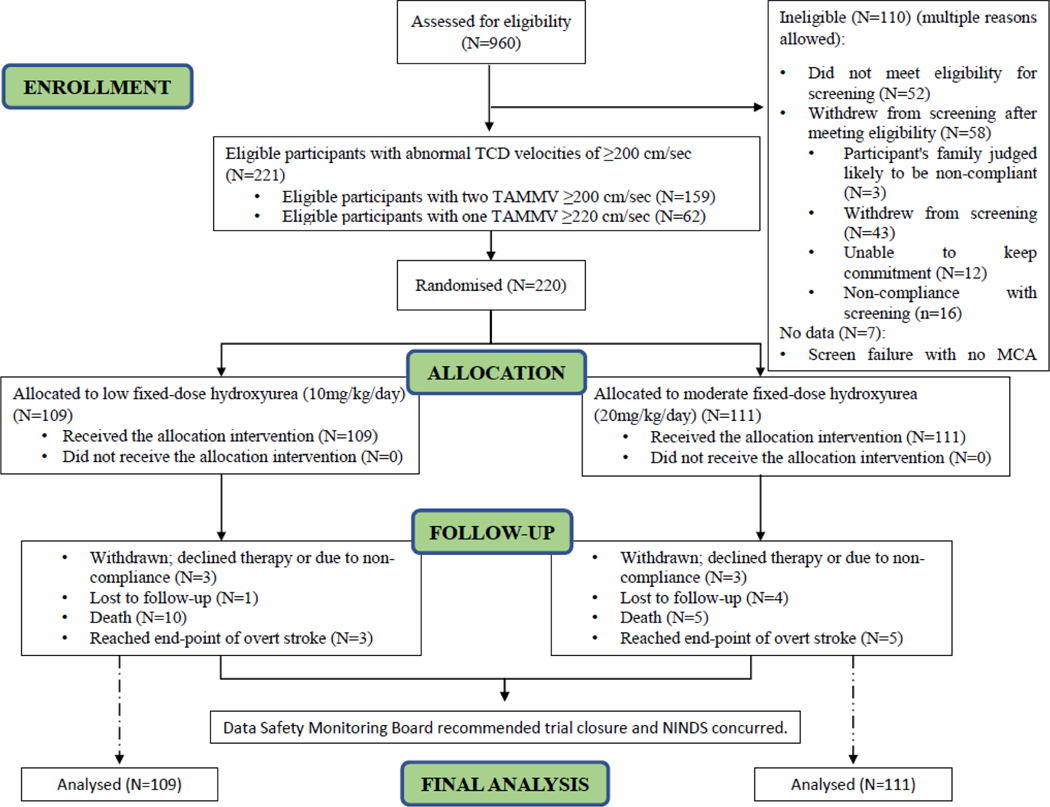
Methods: SPRING is a double-blind, parallel-group, randomised, controlled, phase 3 trial of children aged 5-12 years with sickle cell anaemia with abnormal transcranial Doppler velocities conducted at three teaching hospitals in Nigeria. For randomisation, we used a permuted block allocation scheme with block sizes of four, stratified by sex and site. Allocation was concealed from all but the pharmacists and statisticians. Participants were assigned in a 1:1 ratio to low-dose (10 mg/kg per day) or moderate-dose (20 mg/kg per day) oral hydroxyurea taken once daily with monthly clinical evaluation and laboratory monitoring. The primary outcome was initial stroke or transient ischaemic attack, centrally adjudicated. The secondary outcome was all-cause hospitalisation. We used the intention-to-treat population for data analysis. The trial was stopped early for futility after a planned minimum follow-up of 3·0 years to follow-up for participants. This trial was registered with ClinicalTrials.gov, number NCT02560935.
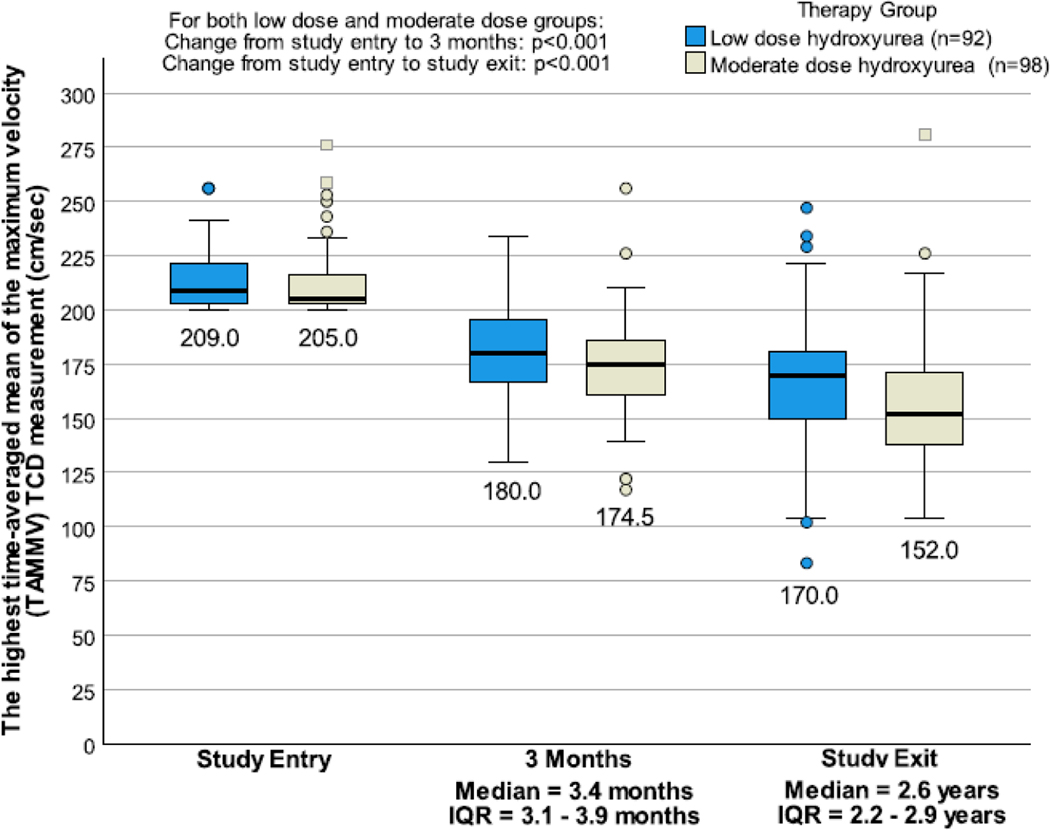
Findings: Between Aug 2, 2016, and June 14, 2018, 220 participants (median age 7·2 years [IQR 5·5-8·9]; 114 [52%] female) were randomly allocated and followed for a median of 2·4 years (IQR 2·0-2·8). All participants were Nigerian and were from the following ethnic groups: 179 (82%) people were Hausa, 25 (11%) were Fulani, and 16 (7%) identified as another ethnicity. In the low-dose hydroxyurea group, three (3%) of 109 participants had strokes, with an incidence rate of 1·19 per 100 person-years and in the moderate-dose hydroxyurea group five (5%) of 111 had strokes with an incidence rate of 1·92 per 100 person-years (incidence rate ratio 0·62 [95% CI 0·10-3·20], p=0·77). The incidence rate ratio of hospitalisation for any reason was 1·71 (95% CI 1·15-2·57, p=0·0071), with higher incidence rates per 100 person-years in the low-dose group versus the moderate-dose group (27·43 vs 16·08). No participant had hydroxyurea treatment stopped for myelosuppression.
Interpretation: Compared with low-dose hydroxyurea therapy, participants treated with moderate-dose hydroxyurea had no difference in the stroke incidence rate. However, secondary analyses suggest that the moderate-dose group could lower incidence rates for all-cause hospitalisations. These findings provide an evidence-based guideline for the use of low-dose hydroxyurea therapy for children with sickle cell anaemia at risk of stroke.
Funding: National Institute of Neurological Disorders and Stroke.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Dr. Kirkham received royalties from the MacKeith Press as a result of her contributions to the
Dr. Trevathan served as a member of the NINDS/NIH advisory council.
Dr. DeBaun and his institution are the sponsor of two externally funded research investigator-initiated projects. Global Blood Therapeutics (GBT) will provide funding for the cost of the clinical studies. GBT will not be a co-sponsor of either study. Dr. DeBaun is not receiving any compensation for the conduct of these two-investigator initiated observational studies. Dr. DeBaun is a member of the Global Blood Therapeutics advisory board for a proposed randomized controlled trial for which he receives compensation. Dr. DeBaun is the steering committee for a Novartis-sponsored phase II trial to prevent priapism in men. Dr. DeBaun was a medical advisor for the development of the CTX001 Early Economic Model. Dr. DeBaun provided medical input on the economic model as part of an expert reference group for Vertex/CRISPR CTX001 Early Economic Model in 2020. Dr. DeBaun provided a one-time consultation to the Formal Pharmaceutical company about sickle cell disease in 2021.
Figures
References
-
- Balkaran B, Char G, Morris JS, Thomas PW, Serjeant BE, Serjeant GR. Stroke in a cohort of patients with homozygous sickle cell disease. J Pediatr 1992; 120(3): 360–6. - PubMed
-
- Ohene-Frempong K, Weiner SJ, Sleeper LA, et al. Cerebrovascular Accidents in Sickle Cell Disease: Rates and Risk Factors. Blood 1998; 91(1): 288–94. - PubMed
-
- Adams RJ, McKie VC, Hsu L, et al. Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. N Engl J Med 1998; 339(1): 5–11. - PubMed
-
- Lagunju IA, Brown BJ, Sodeinde OO. Chronic blood transfusion for primary and secondary stroke prevention in Nigerian children with sickle cell disease: a 5-year appraisal. Pediatr Blood Cancer 2013; 60(12): 1940–5. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
