

Symptom burden and quality of life in patients with high-risk essential thrombocythaemia and polycythaemia vera receiving hydroxyurea or pegylated interferon alfa-2a: a post-hoc analysis of the MPN-RC 111 and 112 trials
- PMID: 34971581
- PMCID: PMC9098160
- DOI: 10.1016/S2352-3026(21)00343-4
Symptom burden and quality of life in patients with high-risk essential thrombocythaemia and polycythaemia vera receiving hydroxyurea or pegylated interferon alfa-2a: a post-hoc analysis of the MPN-RC 111 and 112 trials
Abstract
Background: Patients with essential thrombocythaemia or polycythaemia vera have several symptoms that can worsen their quality of life. We aimed to assess how symptom burden changes over time with cytoreductive therapy.
Methods: We performed a post-hoc analysis of data from MPN-RC 111-a single-arm, open-label, phase 2, multicentre trial at 17 hospitals and cancer centres in Italy and the USA, evaluating the clinical-haematological response to pegylated interferon alfa-2a in patients who were resistant or intolerant to hydroxyurea (NCT01259817)-and MPN-RC 112-a randomised, open-label, phase 3, multicentre trial at 25 hospitals and cancer centres in France, Germany, Israel, Italy, the UK, and the USA, comparing the clinical-haematological response to pegylated interferon alfa-2a versus hydroxyurea in therapy-naive patients with either high-risk essential thrombocythaemia or polycythaemia vera (NCT01258856). Patients completed the Myeloproliferative Neoplasm Symptom Assessment Form (MPN-SAF) and the European Organisation for the Research and Treatment of Cancer Core Quality of Life Questionnaire through 12 months after initiation of treatment as secondary endpoints. In this post-hoc analysis, we examined the association of symptom burden with the clinical-haematological response at 12 months and the effect of baseline symptom burden (ie, high burden [total symptom score ≥20] vs low burden [total symptom score <20]) on subsequent changes in symptoms, estimated via mixed models. A clinically significant improvement in symptom burden was defined as 50% or greater improvement in the MPN-SAF total symptom score from baseline to 12 months in patients with a total symptom score greater than zero at baseline.
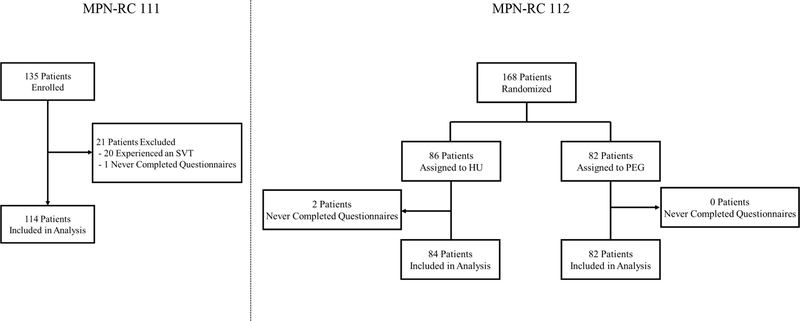
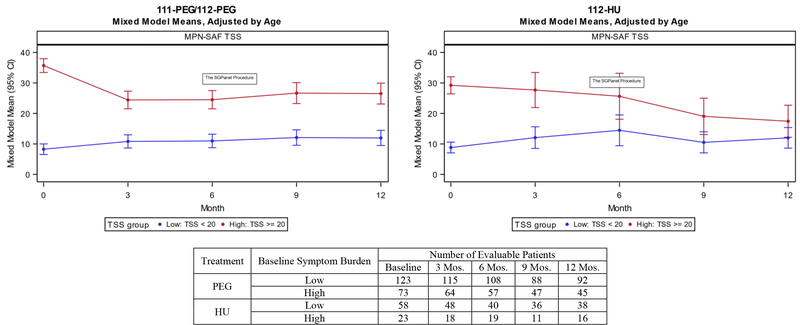
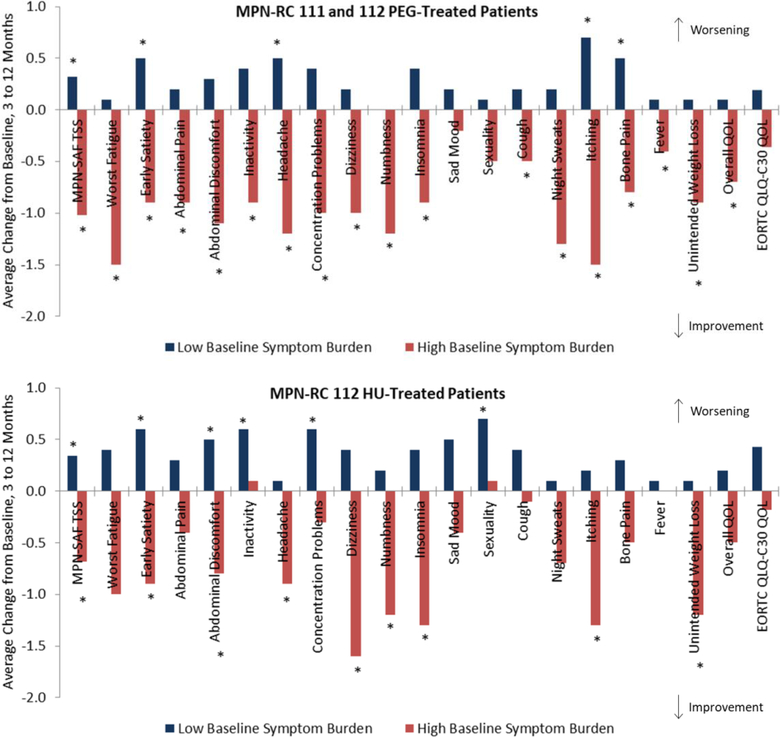
Findings: 135 patients were enrolled in MPN-RC 111 between Feb 15, 2012, and Dec 23, 2015, and 168 were enrolled in MPN-RC 112 between Sept 24, 2011, and June 30, 2016. For this analysis, we included data from 114 patients from MPN-RC 111 (64 [56%] with essential thrombocythaemia and 50 [44%] with polycythaemia vera; 56 [49%] were female, and 100 [91%] of 110 were white) and 166 patients from MPN-RC 112 (79 [48%] with essential thrombocythaemia and 87 [52%] with polycythaemia vera; 68 [41%] were female, and 145 [93%] of 156 were white). At 12 months, a clinically significant improvement in symptom burden was reported by 12 (32%) of 38 complete responders and seven (20%) of 35 partial responders treated with pegylated interferon alfa-2a in MPN-RC 111; five (19%) of 27 complete responders and six (18%) of 34 partial responders treated with pegylated interferon alfa-2a in MPN-112; and eight (27%) of 30 complete responders and six (22%) of 27 partial responders treated with hydroxyurea in MPN-112. More complete and partial responders reported a clinically significant improvement than did non-responders (44 [22%] of 191 complete and partial responders vs four [5%] of 76 non-responders; Fisher's exact p=0·0003). Symptom burden improved between 3 and 12 months in patients with high baseline symptom burden, both those treated with pegylated interferon alfa-2a (mean total symptom score change -10·2, 95% CI -13·2 to -7·2) and those treated with hydroxyurea (-6·8, -11·2 to -2·4). However, symptom burden worsened between 3 and 12 months in patients with low baseline symptom burden (patients treated with pegylated interferon alfa-2a: mean total symptom score change 3·2, 95% CI 0·9 to 5·4; patients treated with hydroxyurea: 3·4, 0·6 to 6·2).
Interpretation: Results can inform treatment decisions, including treatment timing and goals in managing essential thrombocythaemia and polycythaemia vera, because measuring symptom burden from the patient perspective is crucial to understanding treatment efficacy and tolerability.
Funding: US National Cancer Institute of the National Institutes of Health, and Roche Genentech.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests JM reports funding from PharmaEssentia and consulting fees from PharmaEssentia. RAM reports funding from Celgene, Incyte, AbbVie, Samus, Genotech, Promedior, CTI, and Constellation; and consulting fees from Novartis, Sierra Onc, LaJolla, Pharma, and Constellation. All other authors declare no competing interests.
Figures
Similar articles
-
Pegylated interferon alfa-2a in patients with essential thrombocythaemia or polycythaemia vera: a post-hoc, median 83 month follow-up of an open-label, phase 2 trial.Lancet Haematol. 2017 Apr;4(4):e165-e175. doi: 10.1016/S2352-3026(17)30030-3. Epub 2017 Mar 11. Lancet Haematol. 2017. PMID: 28291640 Free PMC article. Clinical Trial.
-
Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): a randomised, non-inferiority, phase 3 trial and its extension study.Lancet Haematol. 2020 Mar;7(3):e196-e208. doi: 10.1016/S2352-3026(19)30236-4. Epub 2020 Jan 31. Lancet Haematol. 2020. PMID: 32014125 Clinical Trial.
-
Long-term efficacy and safety of ruxolitinib versus best available therapy in polycythaemia vera (RESPONSE): 5-year follow up of a phase 3 study.Lancet Haematol. 2020 Mar;7(3):e226-e237. doi: 10.1016/S2352-3026(19)30207-8. Epub 2020 Jan 23. Lancet Haematol. 2020. PMID: 31982039 Free PMC article. Clinical Trial.
-
Appropriate management of polycythaemia vera with cytoreductive drug therapy: European LeukemiaNet 2021 recommendations.Lancet Haematol. 2022 Apr;9(4):e301-e311. doi: 10.1016/S2352-3026(22)00046-1. Lancet Haematol. 2022. PMID: 35358444 Review.
-
Interferons in the treatment of myeloproliferative neoplasms.Ther Adv Hematol. 2024 Feb 19;15:20406207241229588. doi: 10.1177/20406207241229588. eCollection 2024. Ther Adv Hematol. 2024. PMID: 38380373 Free PMC article. Review.
Cited by
-
Structural and Dynamic Differences between Calreticulin Mutants Associated with Essential Thrombocythemia.Biomolecules. 2023 Mar 10;13(3):509. doi: 10.3390/biom13030509. Biomolecules. 2023. PMID: 36979444 Free PMC article.
-
Identification of Novel Risk Variants of Inflammatory Factors Related to Myeloproliferative Neoplasm: A Bidirectional Mendelian Randomization Study.Glob Med Genet. 2024 Feb 12;11(1):48-58. doi: 10.1055/s-0044-1779665. eCollection 2024 Jan. Glob Med Genet. 2024. PMID: 38348158 Free PMC article.
-
Novel therapeutic strategies for essential thrombocythemia/polycythemia vera.Blood Res. 2023 Apr 30;58(S1):83-89. doi: 10.5045/br.2023.2023013. Blood Res. 2023. PMID: 37105562 Free PMC article. Review.
-
New approaches to standard of care in early-phase myeloproliferative neoplasms: can interferon-α alter the natural history of the disease?Haematologica. 2025 Apr 1;110(4):850-862. doi: 10.3324/haematol.2023.283958. Epub 2024 Oct 24. Haematologica. 2025. PMID: 39445431 Free PMC article. Review.
-
Research trends in essential thrombocythemia from 2001 to 2024: a bibliometric analysis.Discov Oncol. 2025 Apr 15;16(1):528. doi: 10.1007/s12672-025-02232-9. Discov Oncol. 2025. PMID: 40232559 Free PMC article.
References
-
- Scherber R, Dueck AC, Johansson P, et al. The Myeloproliferative Neoplasm Symptom Assessment Form (MPN-SAF): International prospective validation and reliability trial in 402 patients. Blood 2011; 118(2): 401–8. - PubMed
-
- Barosi G, Birgegard G, Finazzi G, et al. Response criteria for essential thrombocythemia and polycythemia vera: result of a European LeukemiaNet consensus conference. Blood 2009; 113(20): 4829–33. - PubMed
-
- Barosi G, Besses C, Birgegard G, et al. A unified definition of clinical resistance/intolerance to hydroxyurea in essential thrombocythemia: results of a consensus process by an international working group. Leukemia 2007; 21(2): 277–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
