

Community seroprevalence and risk factors for SARS-CoV-2 infection in different subpopulations in Vellore, India, and their implications for future prevention
- PMID: 34971822
- PMCID: PMC8712712
- DOI: 10.1016/j.ijid.2021.12.356
Community seroprevalence and risk factors for SARS-CoV-2 infection in different subpopulations in Vellore, India, and their implications for future prevention
Abstract
Objectives: The aim of this study was to inform public health policy decisions through the assessment of IgG antibody seroprevalence in the population and the risk factors for SARS-CoV-2 infection.
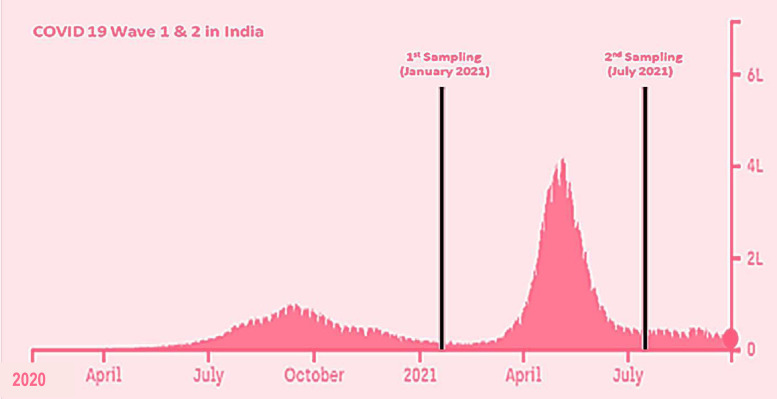
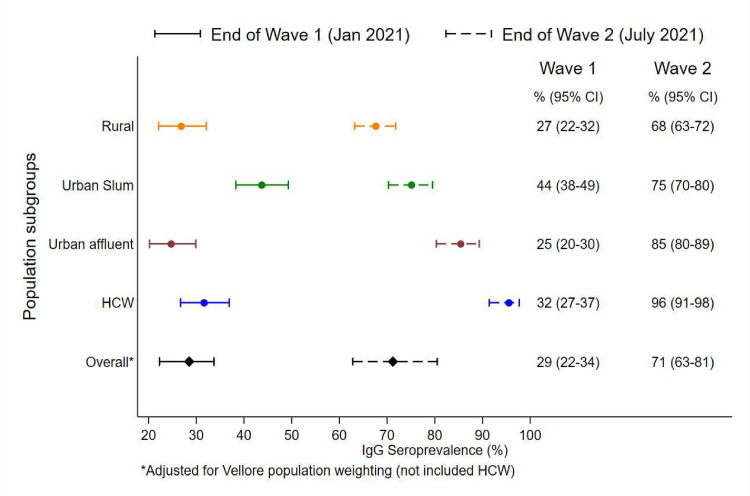
Methods: The seroprevalence of IgG antibodies among different subpopulations at the end of the first and second waves of the pandemic was estimated. Various risk factors associated with seropositivity, including sociodemography, IgG antibodies against endemic human coronavirus, and vaccination status, were also assessed.
Results: For all 2433 consenting participants, the overall estimated seroprevalences at the end of first and second waves were 28.5% (95% CI 22.3-33.7%) and 71.5% (95% CI 62.8-80.5%), respectively. The accrual of IgG positivity was heterogeneous, with the highest seroprevalences found in urban slum populations (75.1%). Vaccine uptake varied among the subpopulations, with low rates (< 10%) among rural and urban slum residents. The majority of seropositive individuals (75%) were asymptomatic. Residence in urban slums (OR 2.02, 95% CI 1.57-2.6; p < 0.001), middle socioeconomic status (OR 1.77, 95% CI 1.17-2.67; p = 0.007), presence of diabetes (OR 1.721, 95% CI 1.148-2.581; p = 0.009), and hypertension (OR 1.75, 95% CI 1.16-2.64; p = 0.008) were associated with seropositivity in multivariable analyses.
Conclusion: Although considerable population immunity has been reached, with more than two-thirds seropositive, improved vaccination strategies among unreached subpopulations and high-risk individuals are suggested for better preparedness in future.
Keywords: COVID; India; SARS-CoV-2; Seroprevalence.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors have no conflicts of interest to declare.
Figures

References
-
- Anand A, Sandefur J, Subramanian A. Three new estimates of deaths in India during the pandemic. Center for Global Development. Jul 20, 2021. https://www.cgdev.org/blog/three-new-estimates-deaths-during-pandemic.
-
- Anderson EM, Goodwin EC, Verma A, Arevalo CP, Bolton MJ, Weirick ME, UPenn COVID Processing Unit. Betts MR, Wherry EJ, Meyer NJ, Cherry S, Bates P, Rader DJ, Hensley SE. Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection. Cell. 2021;184(7) doi: 10.1016/j.cell.2021.02.010. et al. 1858–64.e10Epub 2021 Feb 9. PMID: 33631096; PMCID: PMC7871851. - DOI - PMC - PubMed
-
- Covid19India.org (accessed on September 30, 2021 ).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
