

Validation of visual estimation of neonatal jaundice in low-income and middle-income countries: a multicentre observational cohort study
- PMID: 34972760
- PMCID: PMC8720979
- DOI: 10.1136/bmjopen-2020-048145
Validation of visual estimation of neonatal jaundice in low-income and middle-income countries: a multicentre observational cohort study
Abstract
Objective: Determine the sensitivity and specificity of neonatal jaundice visual estimation by primary healthcare workers (PHWs) and physicians as predictors of hyperbilirubinaemia.
Design: Multicentre observational cohort study.
Setting: Hospitals in Chandigarh and Delhi, India; Dhaka, Bangladesh; Durban, South Africa; Kumasi, Ghana; La Paz, Bolivia.
Participants: Neonates aged 1-20 days (n=2642) who presented to hospitals for evaluation of acute illness. Infants referred for any reason from another health facility or those needing immediate cardiopulmonary resuscitation were excluded.
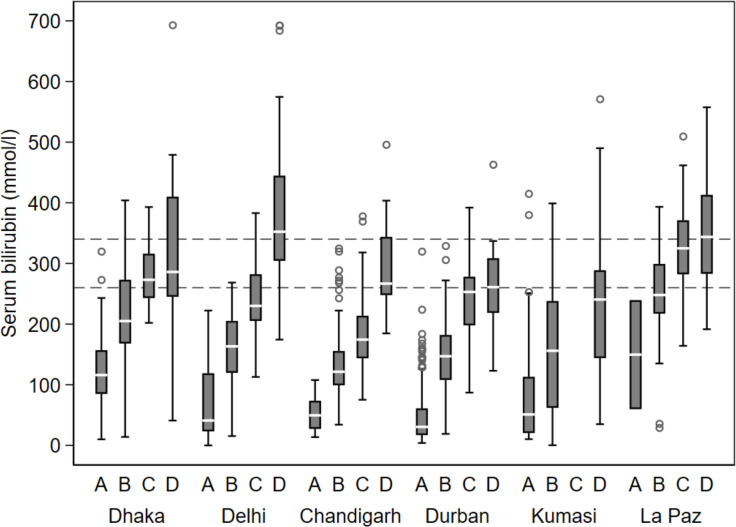
Outcome measures: Infants were evaluated for distribution (head, trunk, distal extremities) and degree (mild, moderate, severe) of jaundice by PHWs and physicians. Serum bilirubin level was determined for infants with jaundice, and analyses of sensitivity and specificity of visual estimations of jaundice used bilirubin thresholds of >260 µmol/L (need for phototherapy) and >340 µmol/L (need for emergency intervention in at-risk and preterm babies).
Results: 1241 (47.0%) neonates had jaundice. High sensitivity for detecting neonates with serum bilirubin >340 µmol/L was found for 'any jaundice of the distal extremities (palms or soles) OR deep jaundice of the trunk or head' for both PHWs (89%-100%) and physicians (81%-100%) across study sites; specificity was more variable. 'Any jaundice of the distal extremities' identified by PHWs and physicians had sensitivity of 71%-100% and specificity of 55%-95%, excluding La Paz. For the bilirubin threshold >260 µmol/L, 'any jaundice of the distal extremities OR deep jaundice of the trunk or head' had the highest sensitivity across sites (PHWs: 58%-93%, physicians: 55%-98%).
Conclusions: In settings where serum bilirubin cannot be measured, neonates with any jaundice on the distal extremities should be referred to a hospital for evaluation and management, where delays in serum bilirubin measurement and appropriate treatment are anticipated following referral, the higher sensitivity sign, any jaundice on the distal extremities or deep jaundice of the trunk or head, may be preferred.
Keywords: community child health; epidemiology; neonatology; primary care; public health.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: RB and MW are WHO staff members. MW contributed to study design, implementation, data analysis and manuscript writing and RB contributed to data analysis and manuscript writing. The opinions expressed in this paper do not necessarily represent the position of the WHO. The funding agencies did not influence the conduct or outcomes of the study, data analysis or interpretation, or preparation of this paper. The authors declare no other potential competing interests.
Figures
References
-
- Ip S, Chung M, Kulig J. American Academy of pediatric technical report. an evidence-based review of important issues concerning neonatal hyperbilirubinemia. Pediatrics 2004;114:e130-153. 3. Totapally BR, Torbati D. Neonatal jaundice. Int Pediatr 2005;20:47–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources