

Risk factors for Coronavirus disease-associated mucormycosis
- PMID: 34974056
- PMCID: PMC8717704
- DOI: 10.1016/j.jinf.2021.12.039
Risk factors for Coronavirus disease-associated mucormycosis
Abstract
Background: The epidemiology of the Coronavirus-disease associated mucormycosis (CAM) syndemic is poorly elucidated. We aimed to identify risk factors that may explain the burden of cases and help develop preventive strategies.
Methods: We performed a case-control study comparing cases diagnosed with CAM and taking controls as recovered COVID 19 patients who did not develop mucormycosis. Information on comorbidities, glycemic control, and practices related to COVID-19 prevention and treatment was recorded. Multivariate regression analysis was used to identify independent predictors.
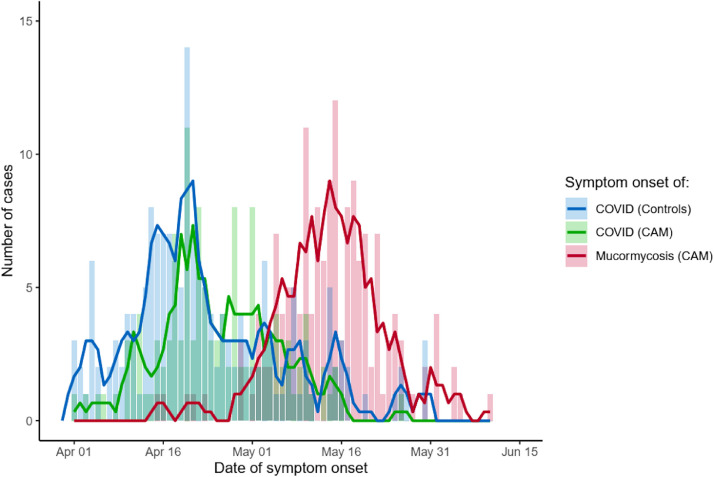
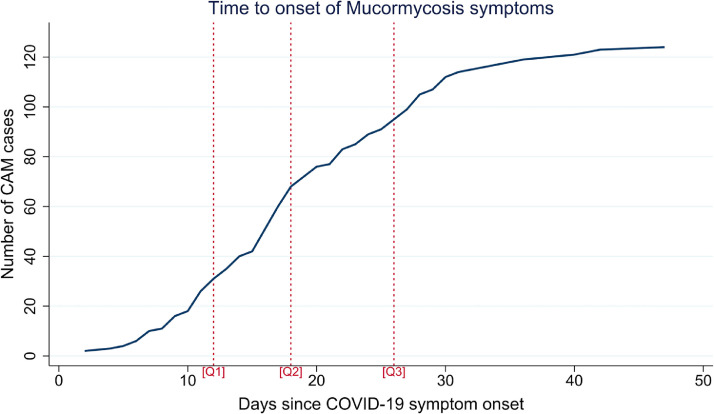
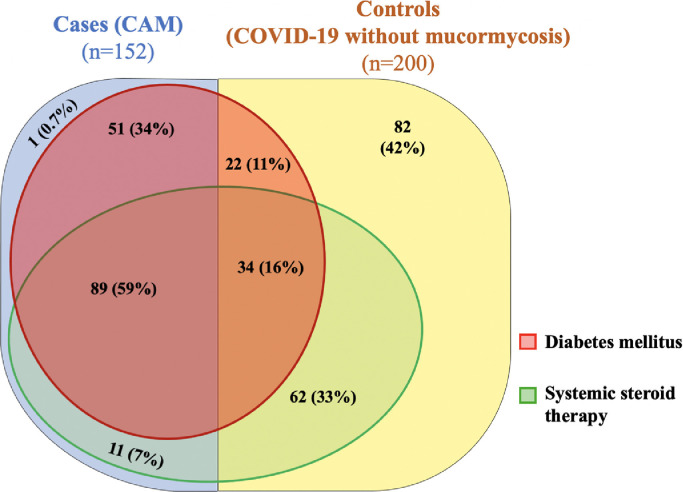
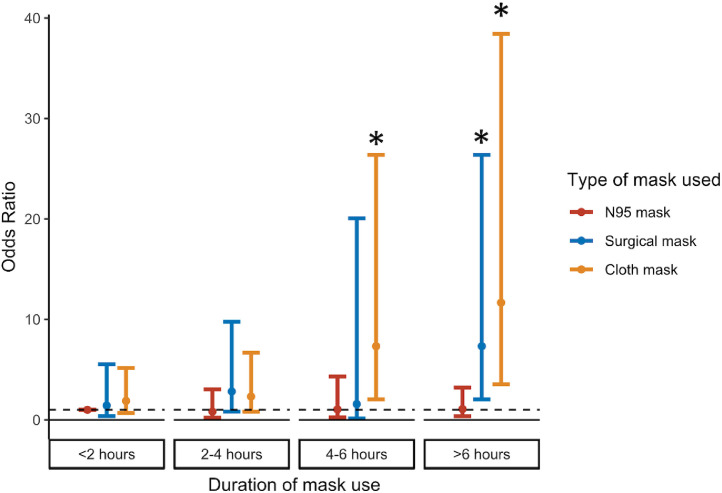
Results: A total of 352 patients (152 cases and 200 controls) diagnosed with COVID-19 during April-May 2021 were included. In the CAM group, symptoms of mucormycosis began a mean of 18.9 (SD 9.1) days after onset of COVID-19, and predominantly rhino-sinus and orbital involvement was present. All, but one, CAM cases had conventional risk factors of diabetes and steroid use. On multivariable regression, increased odds of CAM were associated with the presence of diabetes (adjusted OR 3.5, 95% CI 1.1-11), use of systemic steroids (aOR 7.7, 95% CI 2.4-24.7), prolonged use of cloth and surgical masks (vs. no mask, aOR 6.9, 95%CI 1.5-33.1), and repeated nasopharyngeal swab testing during the COVID-19 illness (aOR 1.6, 95% CI 1.2-2.2). Zinc therapy was found to be protective (aOR 0.05, 95%CI 0.01-0.19). Notably, the requirement of oxygen supplementation or hospitalization did not affect the risk of CAM.
Conclusion: Judicious use of steroids and stringent glycemic control are vital to preventing mucormycosis. Use of clean masks, preference for N95 masks if available, and minimizing swab testing after the diagnosis of COVID-19 may further reduce the incidence of CAM.
Keywords: COVID-19; Case control; Mucormycosis; Risk factors.
Copyright © 2021 The British Infection Association. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no competing interests.
Figures
References
-
- Chakrabarti A., Dhaliwal M. Epidemiology of mucormycosis in India. Curr Fungal Infect Rep. 2013;7(4):287–292. Dec 1.
-
- Hindustan Times . Hindustan Times; 2021. Black fungus: here is a list of states with highest number of mucormycosis cases [Internet]https://www.hindustantimes.com/india-news/black-fungus-states-with-highe... [citedJun 21]. Available from.
-
- Cornely O.A., Alastruey-Izquierdo A., Arenz D., Chen S.C.A., Dannaoui E., Hochhegger B., et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019;19(12):e405–e421. Dec. - PMC - PubMed
-
- WHO COVID-19 Case definition [Internet]. [cited 2021 Jun 21]. Available from: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Surveilla...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
