

Daratumumab plus lenalidomide and dexamethasone in transplant-ineligible newly diagnosed multiple myeloma: frailty subgroup analysis of MAIA
- PMID: 34974527
- PMCID: PMC8979809
- DOI: 10.1038/s41375-021-01488-8
Daratumumab plus lenalidomide and dexamethasone in transplant-ineligible newly diagnosed multiple myeloma: frailty subgroup analysis of MAIA
Abstract
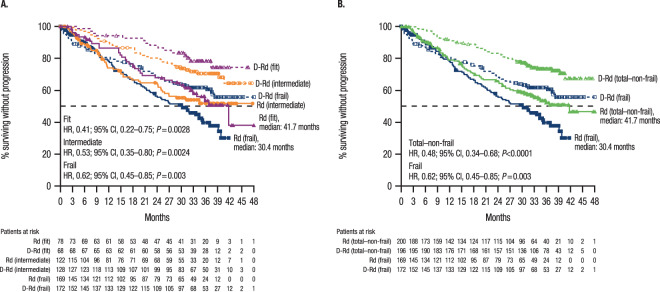
In the phase 3 MAIA study of patients with transplant-ineligible newly diagnosed multiple myeloma (NDMM), daratumumab plus lenalidomide/dexamethasone (D-Rd) improved progression-free survival (PFS) versus lenalidomide/dexamethasone (Rd). We present a subgroup analysis of MAIA by frailty status. Frailty assessment was performed retrospectively using age, Charlson comorbidity index, and baseline Eastern Cooperative Oncology Group performance status score. Patients were classified as fit, intermediate, non-frail (fit + intermediate), or frail. Of the randomized patients (D-Rd, n = 368; Rd, n = 369), 396 patients were non-frail (D-Rd, 196 [53.3%]; Rd, 200 [54.2%]) and 341 patients were frail (172 [46.7%]; 169 [45.8%]). After a 36.4-month median follow-up, non-frail patients had longer PFS than frail patients, but the PFS benefit of D-Rd versus Rd was maintained across subgroups: non-frail (median, not reached [NR] vs 41.7 months; hazard ratio [HR], 0.48; P < 0.0001) and frail (NR vs 30.4 months; HR, 0.62; P = 0.003). Improved rates of complete response or better and minimal residual disease (10-5) negativity were observed for D-Rd across subgroups. The most common grade 3/4 treatment-emergent adverse event in non-frail and frail patients was neutropenia (non-frail, 45.4% [D-Rd] and 37.2% [Rd]; frail, 57.7% and 33.1%). These findings support the clinical benefit of D-Rd in transplant-ineligible NDMM patients enrolled in MAIA, regardless of frailty status.
© 2021. The Author(s).
Conflict of interest statement
TF served in a consulting or advisory role for, served on a speaker’s bureau for, and had travel, accommodations, or other expenses paid or reimbursed by Janssen. GC received honoraria from and served in a consulting or advisory role for Janssen, Celgene, Takeda, and Bristol Myers Squibb; served on a speaker’s bureau for Janssen, Celgene, and Takeda; and received research funding and had travel, accommodations, or other expenses paid or reimbursed by Janssen and Celgene. SZU served in a consulting or advisory role for Amgen, AbbVie, Celgene, Mundipharma, Sanofi, Seattle Genetics, Janssen, Takeda, and SkylineDx; and received grants from Bristol Myers Squibb and Pharmacyclics. CH received honoraria from Celgene, Janssen, Amgen, and Takeda; and had travel, accommodations, or other expenses paid or reimbursed by Celgene, Janssen, and Amgen. SK served in a consulting or advisory role for AbbVie, Celgene, and Kite Pharma. TP served as an advisor for Janssen and Celgene. CT received honoraria from and served in a consulting or advisory role for Janssen, Celgene, Takeda, Amgen, and AbbVie; and had travel, accommodations, or other expenses paid or reimbursed by Janssen, Takeda, Amgen, and AbbVie. NJB received honoraria from and served in a consulting or advisory role for Celgene, Janssen, AbbVie, Amgen, Sanofi, and Takeda; had travel, accommodations, or other expenses paid or reimbursed by Janssen and Celgene; and received research funding from Celgene. SB has nothing to disclose. HN has nothing to disclose. HG served in a consulting or advisory role for Adaptive Biotechnologies, Amgen, Sanofi, Takeda, Bristol Myers Squibb, Celgene, and Janssen; received research funding from Chugai; received grant support from Mundipharma, Amgen, Sanofi, Takeda, Bristol Myers Squibb, Celgene, Janssen, and Novartis; and received honoraria from Novatis, Bristol Myers Squibb, Celgene, Janssen, Chugai, and Art Tempi. HQ received research funding from Amgen, GlaxoSmithKline, Celgene, Sanofi, and Karyopharm; and served in a consulting or advisory role for Amgen, GlaxoSmithKline, Celgene, Karyopharm, Sanofi, Takeda, and Janssen. MM received research funding from Celgene, Janssen, and Sanofi; and received honoraria from Adaptive Biotechnologies, Amgen, Bristol Myers Squibb, Celgene, Janssen, Takeda, Novartis, and Sanofi. CPV received grant support and honoraria from Janssen and Celgene; and received honoraria from Amgen and Takeda. KW received honoraria from GlaxoSmithKline, Sanofi, Adaptive Biotechnologies, Amgen, Bristol Myers Squibb, Celgene, Janssen, and Takeda; served in a consulting or advisory role for GlaxoSmithKline, Amgen, Adaptive Biotechnologies, Bristol Myers Squibb, Celgene, Janssen, Takeda, Sanofi, and Juno; and received institutional research funding from Amgen, Celgene, Sanofi, and Janssen. NR served in a consulting or advisory role for Amgen, Celgene, Bristol Myers Squibb, Janssen, and Takeda; and received grant support from AstraZeneca. BH has nothing to disclose. KB-M consulted for and received honoraria from Amgen, Celgene, Janssen, and Takeda. LB has nothing to disclose. OD received honoraria from Janssen, Celgene, Amgen, and Takeda; and had travel, accommodations, or other expenses paid or reimbursed by Roche, Takeda, Janssen, Celgene, Amgen, and AbbVie. SM received research funding from Janssen, Celgene, and Amgen. DC has nothing to disclose. JU, HP, RVR, CMU, and RK are employees of Janssen. SZ received research support from Janssen and Takeda; served in a consulting or advisory role for Celgene, Janssen, Takeda, Sanofi, Bristol Myers Squibb, and Oncopeptides; and received research funding from Takeda and Janssen.
Figures
References
-
- Lammerts van Bueren J, Jakobs D, Kaldenhoven N, Roza M, Hiddingh S, Meesters J, et al. Direct in vitro comparison of daratumumab with surrogate analogs of CD38 antibodies MOR03087, SAR650984 and Ab79. Blood. 2014;124:3474. doi: 10.1182/blood.V124.21.3474.3474. - DOI
-
- Overdijk MB, Verploegen S, Bögels M, van Egmond M, Lammerts van Bueren JJ, Mutis T, et al. Antibody-mediated phagocytosis contributes to the anti-tumor activity of the therapeutic antibody daratumumab in lymphoma and multiple myeloma. MAbs. 2015;7:311–21. doi: 10.1080/19420862.2015.1007813. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
