

Long-term survival following definitive radiation therapy for recurrence or oligometastases in gynecological malignancies: A landmark analysis
- PMID: 34974906
- PMCID: PMC9257896
- DOI: 10.1016/j.ygyno.2021.12.022
Long-term survival following definitive radiation therapy for recurrence or oligometastases in gynecological malignancies: A landmark analysis
Abstract
Objective: Radiation therapy (RT) may improve outcomes for patients with oligometastatic cancer. We sought to determine if there are long-term survivors treated with definitive RT for recurrent or oligometastatic gynecological cancer (ROMGC), and to evaluate the clinical and disease characteristics of these patients.
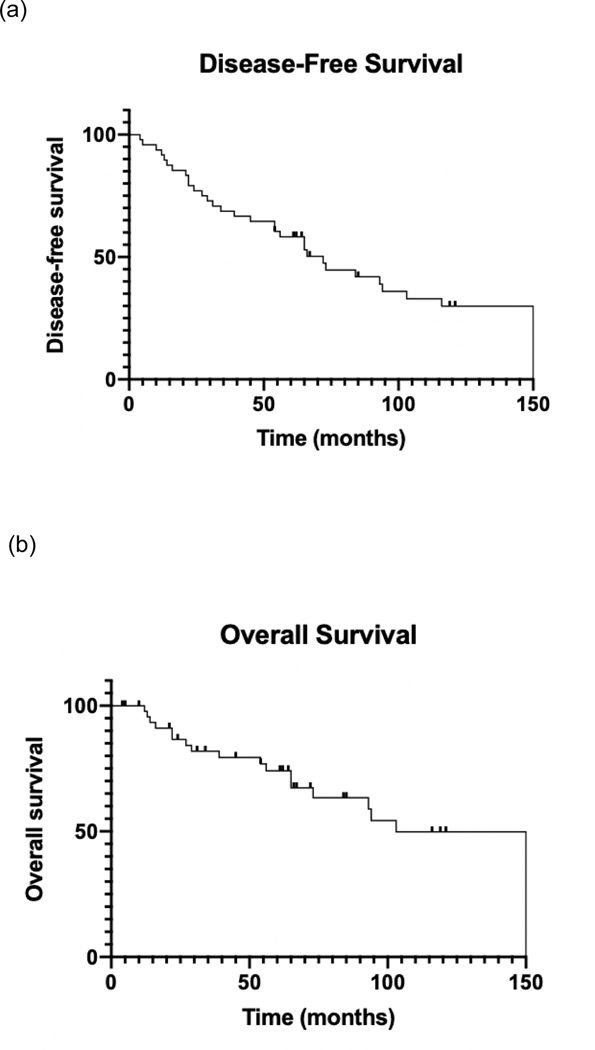
Methods: We performed a landmark analysis in 48 patients with ROMGC who survived for ≥5 years following definitive RT of their metastasis. Patient characteristics were extracted from the medical record. DFS was modeled using the Kaplan-Meier method.
Results: This cohort included 20 patients (42%) with ovarian cancer, 16 (33%) with endometrial cancer, 11 (23%) with cervical cancer, and one (2%) with vaginal cancer. The sites of ROMGC were the pelvic (46%), para-aortic (44%), supraclavicular (7%), mediastinal (4%), axillary (4%) lymph nodes and the lung (5.5%). Median total RT dose and fractionation were 62.1 Gy and 2.1 Gy/fraction; one patient was treated with SBRT. 32 patients (67%) received chemoradiation; these patients had higher rates of median DFS than those treated with RT alone (93 vs. 34 months, P = 0.05). At median follow-up of 11.7 years, 11 (23%) patients had progression of disease. 20 (42%) patients had died, 9 (19%) died from non-gynecologic cancer and 8 (17%) from gynecologic cancer (three were unknown). 25 (52%) patients were alive and disease-free (10 initially had endometrial cancer [63% of these patients], eight had cervical cancer [73%], six had ovarian cancer [30%], one had vaginal cancer [100%]).
Conclusions: Long-term survival is possible for patients treated with definitive RT for ROMG, however randomized data are needed to identify which patients derive the most benefit.
Keywords: Gynecologic neoplasms; Neoplasm metastasis; Radiotherapy.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest None.
Figures



References
-
- SEER 5-Year Relative Survival Rates, 2011–2017. National Cancer Insitutute;2018.
-
- Bodurka-Bevers D, Morris M, Eifel PJ, et al. Posttherapy surveillance of women with cervical cancer: an outcomes analysis. Gynecol Oncol. 2000;78(2):187–193. - PubMed
-
- Moore KN, Secord AA, Geller MA, et al. Niraparib monotherapy for late-line treatment of ovarian cancer (QUADRA): a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2019;20(5):636–648. - PubMed
-
- Chan JK, Tian C, Teoh D, et al. Survival after recurrence in early-stage high-risk epithelial ovarian cancer: a Gynecologic Oncology Group study. Gynecol Oncol. 2010;116(3):307–311. - PubMed
