

Persistent racial disparities in cervical cancer screening with Pap test
- PMID: 34976700
- PMCID: PMC8684022
- DOI: 10.1016/j.pmedr.2021.101652
Persistent racial disparities in cervical cancer screening with Pap test
Abstract
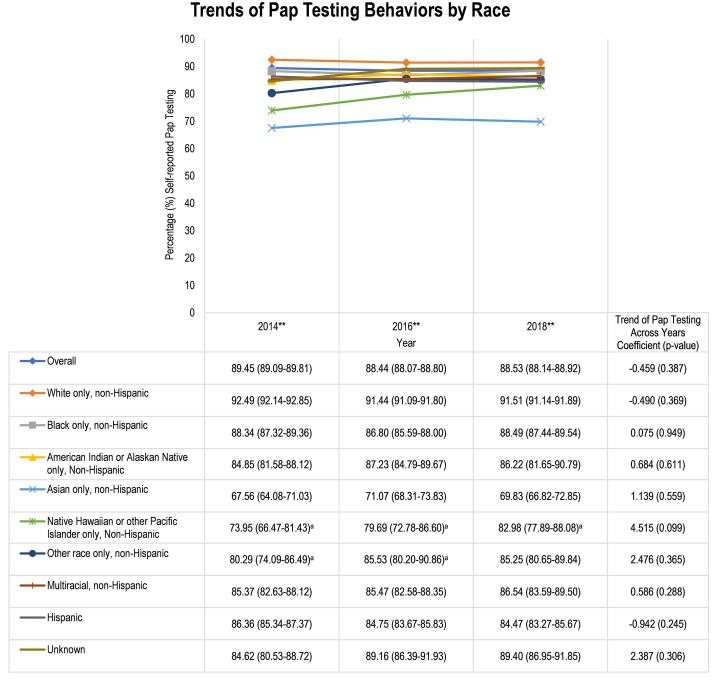
Given the racial disparities in cervical cancer screening, incidence, and mortality, the purpose of this study was to estimate cervical cancer screening behaviors through self-reported Pap testing among racial groups in the U.S. This cross-sectional study utilized the Behavioral Risk Factor Surveillance System (BRFSS) data to compare Pap testing behaviors among women of different racial groups. The BRFSS data from 2014, 2016, and 2018 were chosen because these were the most recent years of data capturing cervical cancer screening information. The primary outcome was self-reported Pap testing behavior (yes/no). Racial groups were analyzed with the original categorical responses for the race/ethnicity variable to investigate Pap testing behaviors across all racial groups. Statistical analyses included descriptive statistics and a multivariable binomial logistic regression model to assess differences of Pap testing by race after adjusting for covariates. Among the 538,218 females included, 88.81% (95% CI: 88.60-89.03) reported receiving a Pap test. Pap testing behaviors differed significantly between racial groups in 2014, 2016, and 2018 (p < 0.001 for all years). Compared to White women, Asians (OR: 0.169, 95% CI: 0.149-0.191), Native Hawaiians/other Pacific Islanders (OR: 0.339, 95% CI: 0.249-0.462), American Indians or Alaskan Natives (OR: 0.664, 95% CI: 0.532-0.829), Hispanics (OR: 0.726, 95% CI: 0.670-0.786), and other non-Hispanic races (OR: 0.439, 95% CI: 0.323-0.598) were significantly less likely to receive Pap test. Racial disparities in cervical cancer screening with Pap tests exist for Asians, Native Hawaiians/other Pacific Islanders, American Indians or Alaskan Natives, Hispanics, and other non-Hispanics.
Keywords: Cervical cancer screening; Health disparities; Pap test; Racial disparities; Women’s health.
© 2021 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: McDaniel was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number TL1TR003106. The content is solely the authors' responsibility and does not necessarily represent the official views of the National Institutes of Health. McDaniel was also supported by the American Foundation for Pharmaceutical Education (AFPE) under the AFPE Pre-Doctoral Fellowship. These sponsors had no role in study design; collection, analysis, and interpretation of data; writing the report; and the decision to submit the report for publication. Hallam, Cadwallader, Lee, and Chou have no relevant conflicts of interest to disclose.
Figures
References
-
- [dataset], Behavioral Risk Factor Surveillance System: Annual Survey Data, 2014, 2016, and 2018. CDC, Atlanta, GA.
-
- BRFSS, 2013. The BRFSS data user guide https://www.cdc.gov/brfss/data_documentation/pdf/UserguideJune2013.pdf (accessed 20 August 2020).
-
- BRFSS, 2018. LLCP 2018 Codebook Report https://www.cdc.gov/brfss/annual_data/2018/pdf/codebook18_llcp-v2-508.pdf (accessed 05 October 2021).
-
- BRFSS, 2019a. Comparability of Data BRFSS 2018 https://www.cdc.gov/brfss/annual_data/2018/pdf/compare-2018-508.pdf (accessed 07 October 2021).
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
