

Coagulation Factor XIII Subunit A Is a Biomarker for Curative Effects and Prognosis in Malignant Solid Tumors, Especially Non-small Cell Lung Cancer
- PMID: 34976787
- PMCID: PMC8714639
- DOI: 10.3389/fonc.2021.719085
Coagulation Factor XIII Subunit A Is a Biomarker for Curative Effects and Prognosis in Malignant Solid Tumors, Especially Non-small Cell Lung Cancer
Abstract
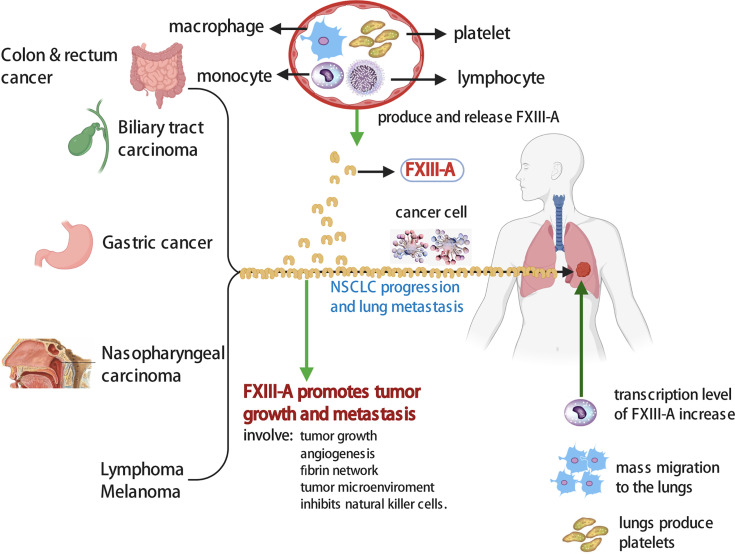
Background: The expression of coagulant factor XIII subunit A (FXIII-A) is significantly increased in some types of cancer cells and tumor-associated macrophages (TAMs). However, few studies on plasma FXIII-A in cancer patients have been conducted and have shown contradictory results, so the relationship of plasma FXIII-A with the progression and prognosis of malignant tumors is still unknown. This study explored the association of plasma FXIII-A with a curative effect and the prognosis of patients with malignant solid tumors.
Methods: We monitored plasma FXIII-A before and during systemic therapy and assessed its relationship with the curative effect and prognosis of malignant solid tumors, especially non-small cell lung carcinoma (NSCLC), by propensity-adjusted, multivariable logistic regression analysis and survival curve, in a prospective study of 1147 patients with different types of malignant solid tumors. The influencing factors of plasma FXIII-A were also analyzed.
Results: We found that D-dimer (D2) = 1 mg/L was the inflection point for the association between FXIII-A and D2: FXIII-A was significantly negatively correlated with D2 (r = -0.39, p < 0.01) and FDP (r = -0.40, p < 0.01) in D2 > 1 mg/L but uncorrelated with D2 or FDP in D2 ≤ 1 mg/L, which provided a method to find a more realistic plasma FXIII-A level. Plasma FXIII-A was positively correlated with age, platelets, lymphocytes, monocytes and carcinoembryonic antigen (CEA). It was found for the first time that plasma FXIII-A was abnormally significantly increased (FXIII-A > 150%) in post-therapy patients, especially in NSCLC and lung metastasis patients, and the incidence of FXIII-A > 150% in lung adenocarcinoma was 16 times higher than that in lung squamous carcinoma. FXIII-A > 150% proved to be an independent risk factor for disease progression in NSCLC patients (OR=5.74, 95% CI: 1.20-27.60, p = 0.029), predicting poor efficacy. The marked decrease in plasma FXIII-A (FXIII-A < 40%) was related to coagulation disorders and poor prognosis with a short survival time (median survival time of 4 months).
Conclusions: Plasma FXIII-A has the potential to be a real-time biomarker with bidirectional indicator effects to assess curative effects and prognosis in malignant solid tumors, especially NSCLC.
Keywords: biomarker; curative effect; factor XIII subunit A; factor XIII/transglutaminases; non-small cell lung cancer; prognosis; tumor-associated macrophages (TAMs).
Copyright © 2021 Luo, Li, Li, Zhang, Deng, Hu, Yan, Zhou and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources