

Tracheal Tube-Mounted Camera Assisted Intubation vs. Videolaryngoscopy in Expected Difficult Airway: A Prospective, Randomized Trial (VivaOP Trial)
- PMID: 34977071
- PMCID: PMC8714897
- DOI: 10.3389/fmed.2021.767182
Tracheal Tube-Mounted Camera Assisted Intubation vs. Videolaryngoscopy in Expected Difficult Airway: A Prospective, Randomized Trial (VivaOP Trial)
Abstract
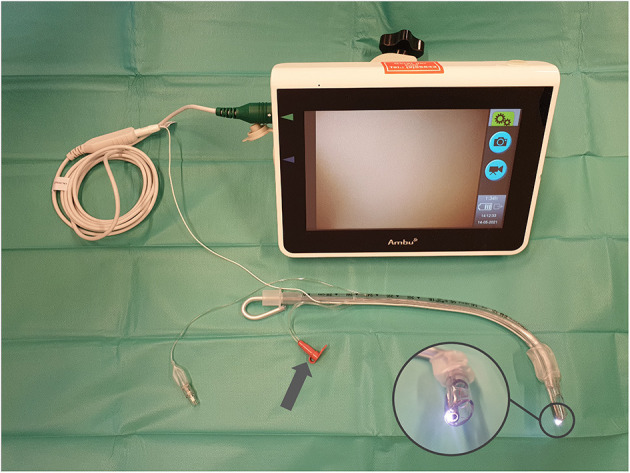
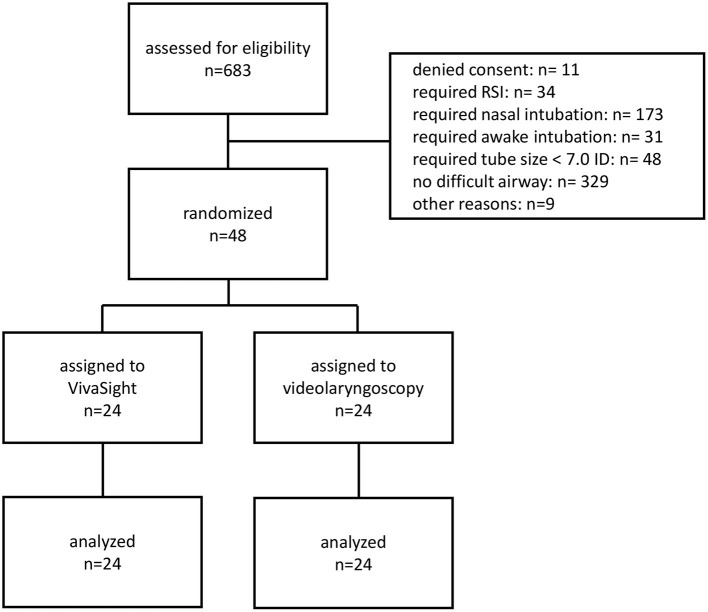
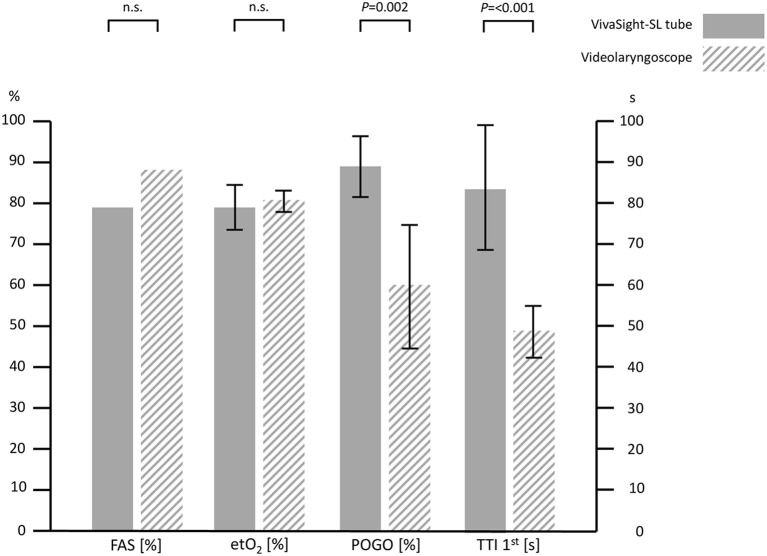
Background: Tracheal intubation in patients with an expected difficult airway may be facilitated by videolaryngoscopy (VL). The VL viewing axis angle is specified by the blade shape and visualization of the larynx may fail if the angle does not meet anatomy of the patient. A tube with an integrated camera at its tip (VST, VivaSight-SL) may be advantageous due to its adjustable viewing axis by means of angulating an included stylet. Methods: With ethics approval, we studied the VST vs. VL in a prospective non-inferiority trial using end-tidal oxygen fractions (etO2) after intubation, first-attempt success rates (FAS), visualization assessed by the percentage of glottis opening (POGO) scale, and time to intubation (TTI) as outcome parameters. Results: In this study, 48 patients with a predicted difficult airway were randomized 1:1 to intubation with VST or VL. Concerning oxygenation, the VST was non-inferior to VL with etO2 of 0.79 ± 0.08 (95% CIs: 0.75-0.82) vs. 0.81 ± 0.06 (0.79-0.84) for the VL group, mean difference 0.02 (-0.07 to 0.02), p = 0.234. FAS was 79% for VST and 88% for VL (p = 0.449). POGO was 89 ± 21% in the VST-group and 60 ± 36% in the VL group, p = 0.002. TTI was 100 ± 57 s in the VST group and 68 ± 65 s in the VL group (p = 0.079). TTI with one attempt was 84 ± 31 s vs. 49 ± 14 s, p < 0.001. Conclusion: In patients with difficult airways, tracheal intubation with the VST is feasible without negative impact on oxygenation, improves visualization but prolongs intubation. The VST deserves further study to identify patients that might benefit from intubation with VST.
Keywords: VivaSight; airway management (MeSH); intubation (intratracheal); laryngoscope and intubation; laryngoscopy; respiration (artificial).
Copyright © 2021 Grensemann, Möhlenkamp, Breitfeld, Tariparast, Peters, Punke, Kluge and Petzoldt.
Conflict of interest statement
JG has received research support from Adroit Surgical, Ambu, ETView, and Infectopharm, and received consultant and lecture fees from Drägerwerk, Fresenius Medical, GE Healthcare, and Smith Medical; SK received research support from Ambu, Daiichi Sankyo, ETView Ltd., Fisher & Paykel, Pfizer, and Xenios, lecture fees from Astra, C.R.Bard, Baxter, Biotest, Cytosorbents, Daiichi Sankyo, Fresenius, Gilead, Mitsubishi Tanabe Pharma, MSD, Pfizer, Philips, and Zoll, and consultant fees from Bayer, Fresenius, Gilead, MSD, and Pfizer; MP received a research grant awarded by Verathon. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Elective Tracheal Intubation With the VieScope-A Prospective Randomized Non-inferiority Pilot Study (VieScOP-Trial).Front Med (Lausanne). 2022 Mar 15;9:820847. doi: 10.3389/fmed.2022.820847. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35372419 Free PMC article.
-
Vie Scope® versus videolaryngoscopy in expected difficult airways: a randomized controlled trial.Can J Anaesth. 2023 Sep;70(9):1486-1494. doi: 10.1007/s12630-023-02534-y. Epub 2023 Aug 3. Can J Anaesth. 2023. PMID: 37537324 Free PMC article. Clinical Trial.
-
Endotracheal tube-mounted camera-assisted intubation versus conventional intubation in intensive care: a prospective, randomised trial (VivaITN).Crit Care. 2018 Sep 22;22(1):235. doi: 10.1186/s13054-018-2152-4. Crit Care. 2018. PMID: 30241488 Free PMC article. Clinical Trial.
-
Videolaryngoscopy versus direct laryngoscopy for nasotracheal intubation: A systematic review and meta-analysis of randomised controlled trials.J Clin Anesth. 2019 Feb;52:6-16. doi: 10.1016/j.jclinane.2018.08.029. Epub 2018 Aug 25. J Clin Anesth. 2019. PMID: 30153543
-
Efficacy and safety of videolaryngoscopy versus direct laryngoscopy in paediatric intubation: A meta-analysis of 27 randomized controlled trials.J Clin Anesth. 2020 Nov;66:109968. doi: 10.1016/j.jclinane.2020.109968. Epub 2020 Jul 6. J Clin Anesth. 2020. PMID: 32645564
Cited by
-
Elective Tracheal Intubation With the VieScope-A Prospective Randomized Non-inferiority Pilot Study (VieScOP-Trial).Front Med (Lausanne). 2022 Mar 15;9:820847. doi: 10.3389/fmed.2022.820847. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35372419 Free PMC article.
-
Vie Scope® versus videolaryngoscopy in expected difficult airways: a randomized controlled trial.Can J Anaesth. 2023 Sep;70(9):1486-1494. doi: 10.1007/s12630-023-02534-y. Epub 2023 Aug 3. Can J Anaesth. 2023. PMID: 37537324 Free PMC article. Clinical Trial.
-
Decision-Making Tool for Planning Camera-Assisted and Awake Intubation in Head and Neck Surgery.JAMA Otolaryngol Head Neck Surg. 2025 Jun 1;151(6):585-594. doi: 10.1001/jamaoto.2025.0538. JAMA Otolaryngol Head Neck Surg. 2025. PMID: 40310618 Free PMC article.
-
Nasendoscopy to Predict Difficult Videolaryngoscopy: A Multivariable Model Development Study.J Clin Med. 2023 May 12;12(10):3433. doi: 10.3390/jcm12103433. J Clin Med. 2023. PMID: 37240540 Free PMC article.
References
-
- Piepho T, Cavus E, Noppens R, Byhahn C, Dörges V, Zwissler B, et al. . S1 Guideline Airwaymanagement, AWMF-Register No. 001/028 (2015). Available online at: https://www.awmf.org/leitlinien/detail/ll/001-028.html
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous