

Case Report: Severe Edema and Marked Weight Gain Induced by Marginal Thiamine Deficiency in a Patient With Alcohol Dependency and Type 2 Diabetes Mellitus
- PMID: 34977103
- PMCID: PMC8714915
- DOI: 10.3389/fnut.2021.675992
Case Report: Severe Edema and Marked Weight Gain Induced by Marginal Thiamine Deficiency in a Patient With Alcohol Dependency and Type 2 Diabetes Mellitus
Abstract
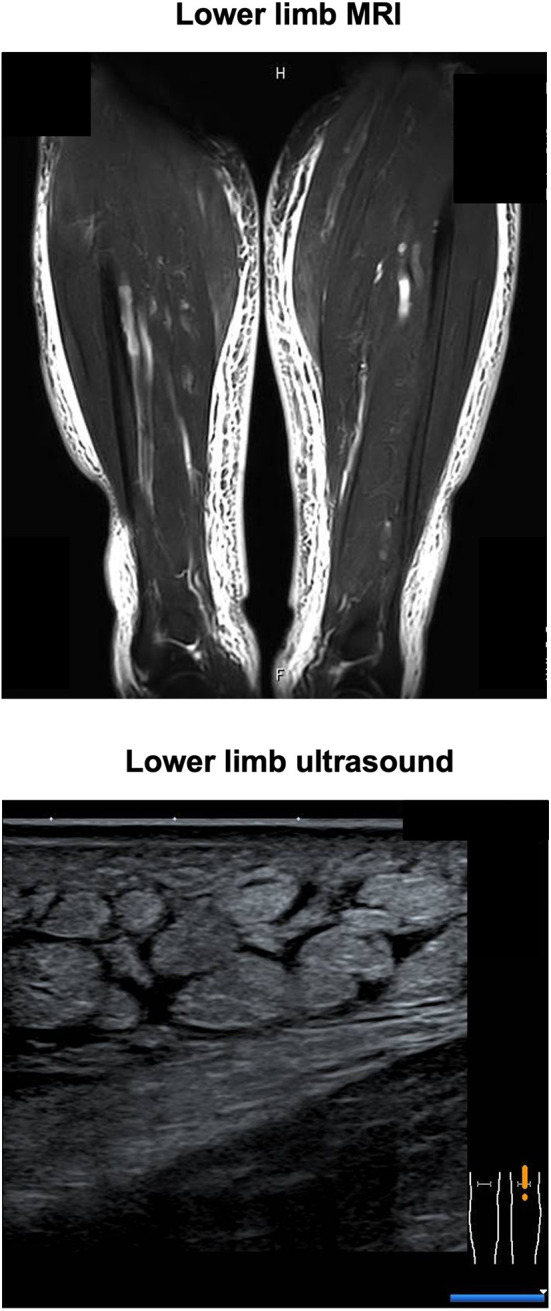
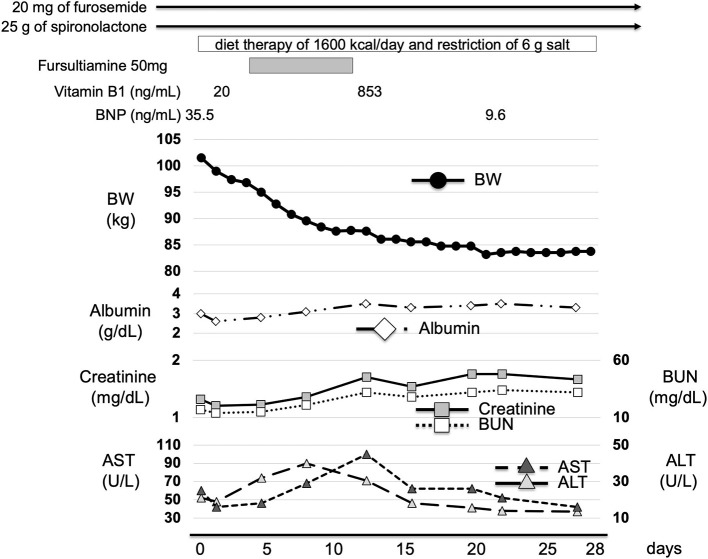
Background: Patients with alcohol use disorder (AUD) may develop peripheral edema due to alcohol-related liver, renal, or heart disease. Thiamine deficiency is reported to occur in AUD and type 2 diabetes mellitus (T2DM). Thiamine deficiency may also cause peripheral edema. Thiamine is essential for optimal glucose metabolism through its role as an essential co-factor for key enzymes in intermediary metabolism. Since glucose metabolism worsens under diabetic conditions, it seems that a relative shortage of thiamine may occur more easily in patients with diabetes mellitus. Case Presentation: A 59-year-old Japanese man was admitted to the hospital with severe peripheral edema. His background history included alcohol liver disease (ALD), chronic renal failure (CRF), and T2DM. His body mass index (BMI) at admission was 37.7 kg/m2 and this represented a 30 kg increase in body weight over 2 months. Laboratory investigations showed anemia, liver and renal injury, hyperglycemia, and marginal hypothyroidism. The plasma thiamine diphosphate concentration was 20 ng/mL (reference range: 24-66 ng/mL). Diet therapy of 1,600 kcal/day and intravenous fursultiamine hydrochloride therapy (50 mg/once a day, seven days) was commenced in combination with intravenous diuretics. After one week, the plasma thiamine concentration was 853 ng/mL, and the patient's body weight had reduced by 18 kg. Conclusions: Patients with T2DM and AUD may develop severe peripheral edema in the context of marginal thiamine deficiency. Fursultiamine hydrochloride (50 mg/once a day, seven days) restored normal plasma thiamine concentrations and may have contributed to the rapid resolution of severe peripheral edema in this case. Empirical treatment with thiamine should be considered in patients with severe peripheral edema in the context of AUD and T2DM.
Keywords: alcohol dependency; thiamine deficiency; type 2 diabetes mellitus; weight gain; whole body edema.
Copyright © 2021 Tanaka, Anno, Takenouchi, Iwamoto, Kaneto, Okimoto and Tomoda.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Acute thiamine deficiency in diabetic ketoacidosis: Diagnosis and management.Pediatr Crit Care Med. 2006 Nov;7(6):595-9. doi: 10.1097/01.PCC.0000244463.59230.DA. Pediatr Crit Care Med. 2006. PMID: 17006386
-
Elevated liver enzymes and fasting glucose levels correlate with neuropathy in patients diagnosed with alcohol use disorder independently of the blood thiamine levels.Alcohol Alcohol. 2024 Jan 17;59(2):agae011. doi: 10.1093/alcalc/agae011. Alcohol Alcohol. 2024. PMID: 38469882
-
Outbreak of life-threatening thiamine deficiency in infants in Israel caused by a defective soy-based formula.Pediatrics. 2005 Feb;115(2):e233-8. doi: 10.1542/peds.2004-1255. Pediatrics. 2005. PMID: 15687431
-
The role of thiamine dependent enzymes in obesity and obesity related chronic disease states: A systematic review.Clin Nutr ESPEN. 2018 Jun;25:8-17. doi: 10.1016/j.clnesp.2018.02.007. Epub 2018 Mar 15. Clin Nutr ESPEN. 2018. PMID: 29779823
-
Decoding Alzheimer's disease from perturbed cerebral glucose metabolism: implications for diagnostic and therapeutic strategies.Prog Neurobiol. 2013 Sep;108:21-43. doi: 10.1016/j.pneurobio.2013.06.004. Epub 2013 Jul 11. Prog Neurobiol. 2013. PMID: 23850509 Review.
References
Publication types
LinkOut - more resources
Full Text Sources