

Pegbelfermin selectively reduces secondary bile acid concentrations in patients with non-alcoholic steatohepatitis
- PMID: 34977519
- PMCID: PMC8689226
- DOI: 10.1016/j.jhepr.2021.100392
Pegbelfermin selectively reduces secondary bile acid concentrations in patients with non-alcoholic steatohepatitis
Abstract
Background & aims: Increased serum bile acids (BAs) have been observed in patients with non-alcoholic steatohepatitis (NASH). Pegbelfermin (PGBF), a polyethylene glycol-modified (PEGylated) analogue of human fibroblast growth factor 21 (FGF21), significantly decreased hepatic steatosis and improved fibrosis biomarkers and metabolic parameters in patients with NASH in a phase IIa trial. This exploratory analysis evaluated the effect of PGBF on serum BAs and explored potential underlying mechanisms.
Methods: Serum BAs and 7α-hydroxy-4-cholesten-3-one (C4) were measured by HPLC-mass spectrometry (MS) using serum collected in studies of patients with NASH (NCT02413372) and in overweight/obese adults (NCT03198182) who received PGBF. Stool samples were collected in NCT03198182 to evaluate faecal BAs by liquid chromatography (LC)-MS and the faecal microbiome by metagenetic and metatranscriptomic analyses.
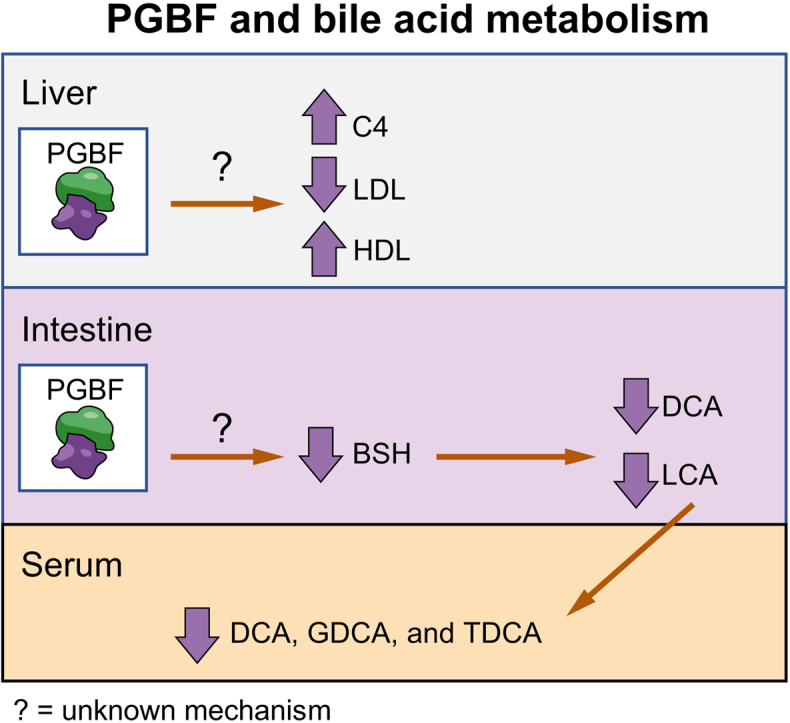
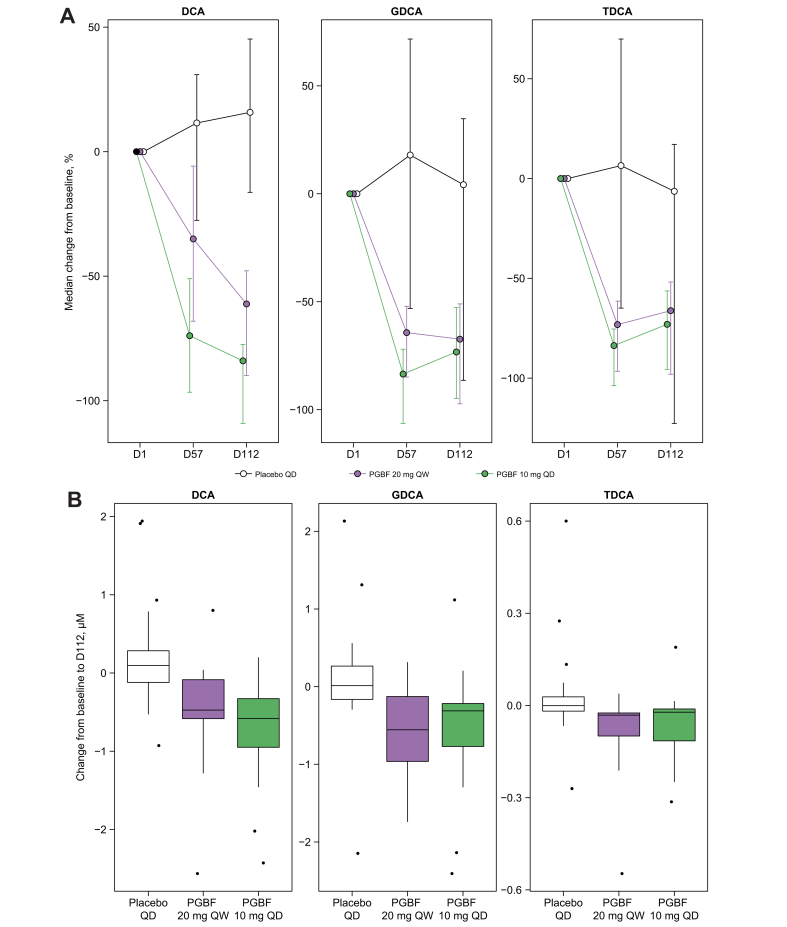
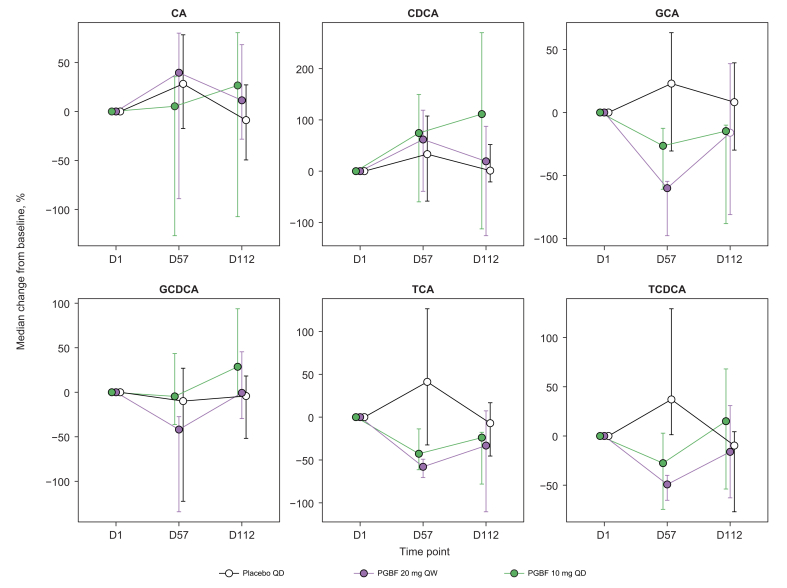
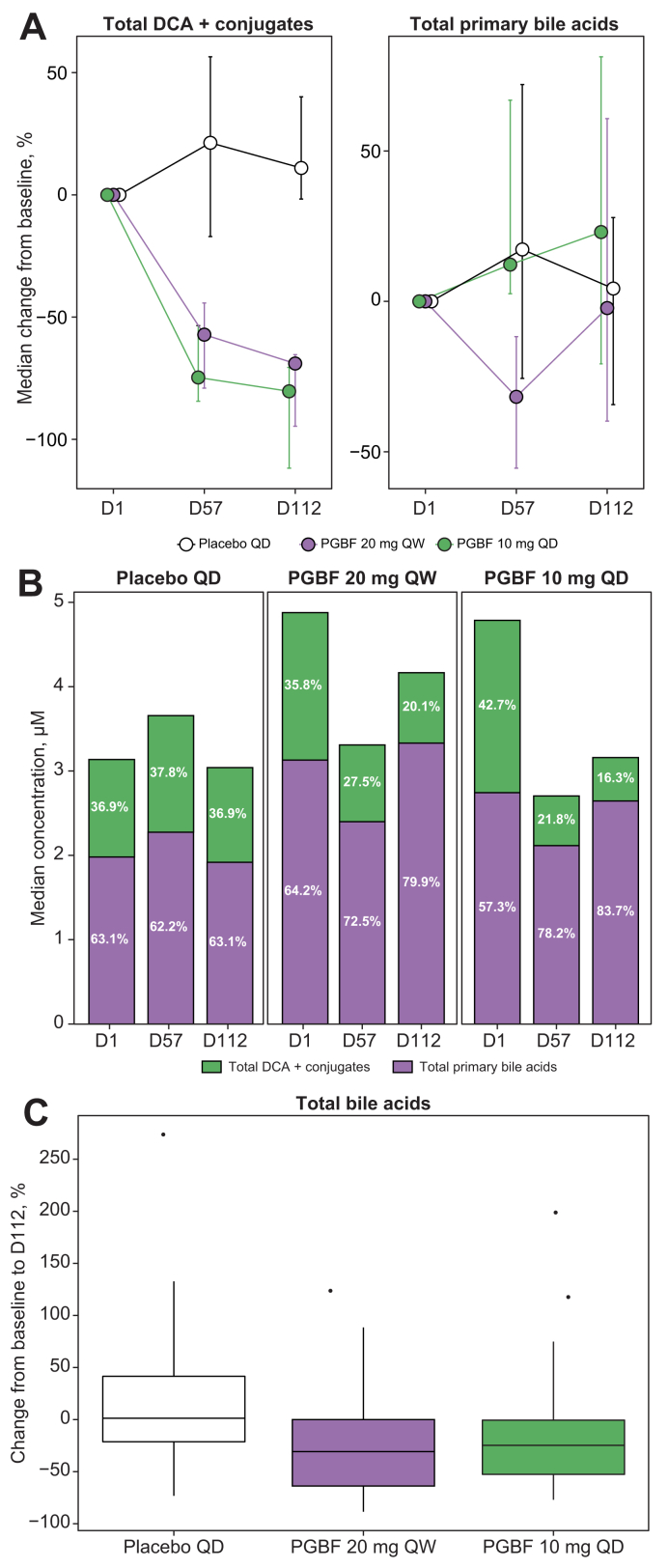
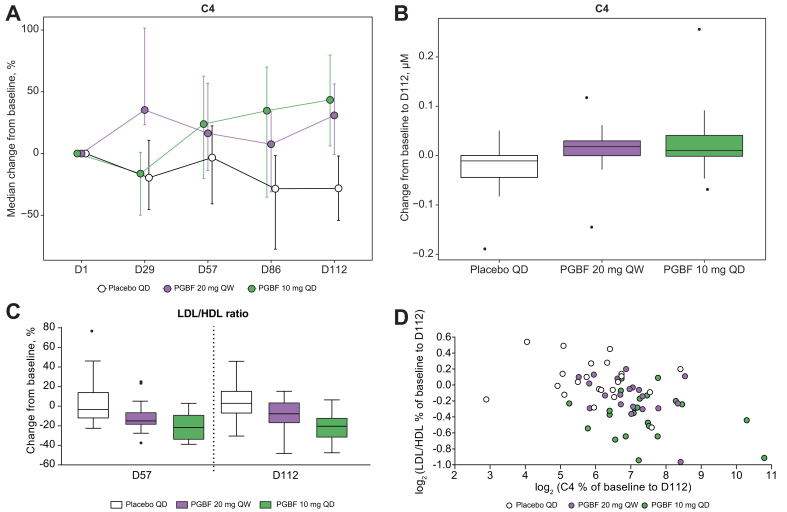
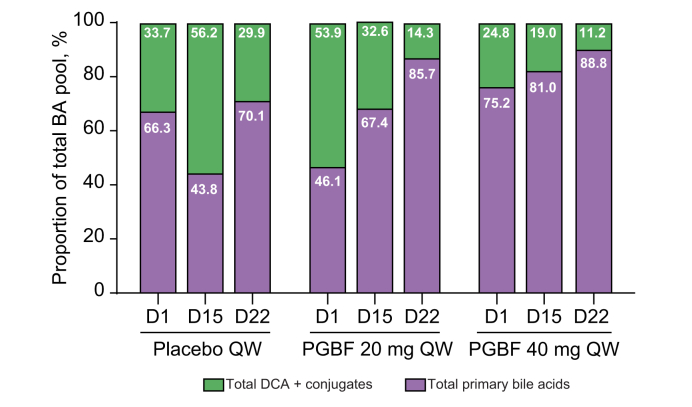
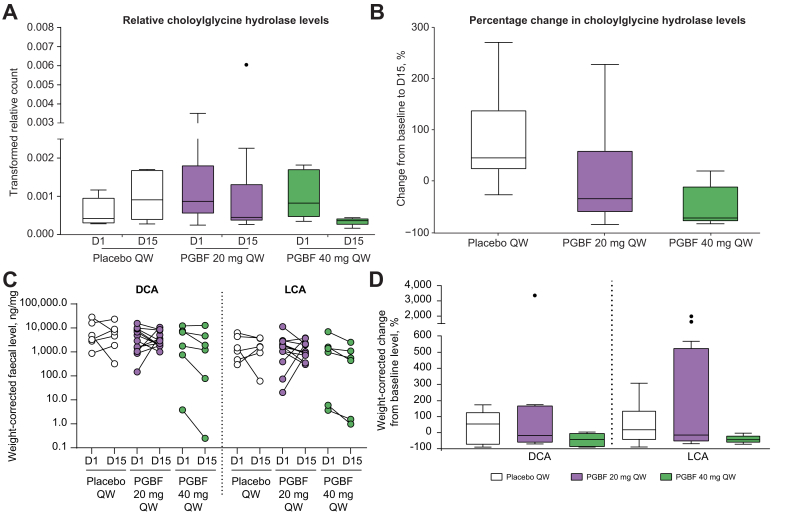
Results: Significant reductions from baseline in serum concentrations of the secondary BA, deoxycholic acid (DCA), and conjugates, were observed with PGBF, but not placebo, in patients with NASH; primary BA concentrations did not significantly change in any arm. Similar effects of PGBF on BAs were observed in overweight/obese adults, allowing for an evaluation of the effects of PGBF on the faecal microbiome and BAs. Faecal transcriptomic analysis showed that the relative abundance of the gene encoding choloylglycine hydrolase, a critical enzyme for secondary BA synthesis, was reduced after PGBF, but not placebo, administration. Furthermore, a trend of reduction in faecal secondary BAs was observed.
Conclusions: PGBF selectively reduced serum concentrations of DCA and conjugates in patients with NASH and in healthy overweight/obese adults. Reduced choloylglycine hydrolase gene expression and decreased faecal secondary BA levels suggest a potential role for PGBF in modulating secondary BA synthesis by gut microbiome. The clinical significance of DCA reduction post-PGBF treatment warrants further investigation.
Lay summary: Pegbelfermin (PGBF) is a hormone that is currently being studied in clinical trials for the treatment of non-alcoholic fatty liver disease. In this study, we show that PGBF treatment can reduce bile acids that have previously been shown to have toxic effects on the liver. Additional studies to understand how PGBF regulates bile acids may provide additional information about its potential use as a treatment for fatty liver.
Keywords: ALT, alanine aminotransferase; AST, aspartate aminotransferase; ApoA1, apolipoprotein A1; BA, bile acid; BSH, bile salt hydrolase; Bile salt hydrolase; Biomarkers; C4; C4, 7α-hydroxy-4-cholesten-3-one; CA, cholic acid; CDCA, chenodeoxycholic acid; CYP7A1, cytochrome P450 7A1; DCA, deoxycholic acid; Deoxycholic acid; FGF21; FGF21, fibroblast growth factor 21; FXR, farnesoid X receptor; GCA, glyco-cholic acid; GCDCA, glyco-chenodeoxycholic acid; GDCA, glyco-deoxycholic acid; GUDCA, glyco-ursodeoxycholic acid; HFF, hepatic fat fraction; HbA1c, glycated haemoglobin; LC, liquid chromatography; LCA, lithocholic acid; MS, mass spectrometry; Microbiome; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; PEGylated, polyethylene glycol-conjugated; PGBF, pegbelfermin; PRO-C3, N-terminal type III collagen propeptide; QD, once daily; QW, once weekly; T2DM, type 2 diabetes mellitus; TCA, tauro-cholic acid; TCDCA, tauro-chenodeoxycholic acid; TDCA, tauro-deoxycholic acid; UDCA, ursodeoxycholic acid; baiCD, 7α-hydroxy-3-oxo-delta4-cholenoic acid oxidoreductase; baiH, 7β-hydroxy-3-oxo-delta4-cholenoic acid oxidoreductase; hdhA, 7-alpha-hydroxysteroid dehydrogenase.
© 2021 The Author(s).
Conflict of interest statement
YL, EDC, DES, CM, PS, AA, and GST are employees of Bristol Myers Squibb and may own company stock. BED was an employee of Bristol Myers Squibb at the time of the study. AJS has been a consultant for and received grants from Allergan, AstraZeneca, Bristol Myers Squibb, Intercept Pharmaceuticals, and Viking Therapeutics; has consulted for AbbVie, Affyimmune Therapeutics, Ardelyx, Chemomab, Conatus Pharmaceuticals, Echosens, Fractyl, Galectin Therapeutics, Immuron, Nitto Denko, Nimbus Therapeutics, Nordic Bioscience, Novo Nordisk, and Synlogic Therapeutics; has received grants from Cumberland Pharmaceuticals, Gilead Sciences, Merck, Mallinckrodt Pharmaceuticals, Novartis, Salix Pharmaceuticals, and Shire; owns stock in Akarna Therapeutics, Durect, Genfit, and Tiziana Life Sciences; and is employed by Sanyal Bioscience. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
References
-
- Chalasani N., Younossi Z., Lavine J.E., Charlton M., Cusi K., Rinella M., et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2018;67:328–357. - PubMed
-
- Younossi Z.M., Koenig A.B., Abdelatif D., Fazel Y., Henry L., Wymer M. Global epidemiology of nonalcoholic fatty liver disease—meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. - PubMed
-
- Legry V., Francque S., Haas J.T., Verrijken A., Caron S., Chávez-Talavera O., et al. Bile acid alterations are associated with insulin resistance, but not with NASH, in obese subjects. J Clin Endocrinol Metab. 2017;102:3783–3794. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
