

SARS-CoV-2 in hospital air as revealed by comprehensive respiratory viral panel sequencing
- PMID: 34977533
- PMCID: PMC8711137
- DOI: 10.1016/j.infpip.2021.100199
SARS-CoV-2 in hospital air as revealed by comprehensive respiratory viral panel sequencing
Abstract
Background: Nosocomially acquired severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) infection has become the most significant pandemic of our lifetime. Though its transmission was essentially attributed to droplets from an infected person, with recent advancements in knowledge, aerosol transmission seems to be a viable pathway, as well. Because of the lower biological load in ambient aerosol, detection of SARS-CoV-2 is challenging. A few recent attempts of sampling large aerosol volumes and using next-generation sequencing (NGS) to detect the presence of SARS-CoV-2 in the air at very low levels gave positive results. These results suggest the potential of using this technique to detect the presence of SARS-CoV-2 and use it as an early warning signal for possible outbreak or recurrence of coronavirus disease 2019 (COVID-19).
Aim: To assess efficacy of comprehensive respiratory viral panel (CRVP) sequencing and RT-PCR for low-level identification of SARS-CoV-2 and other respiratory viruses in indoor air.
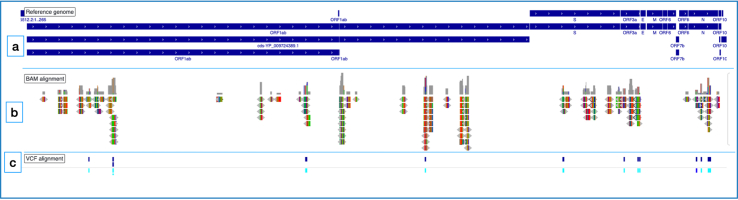
Methods: A large volume of indoor aerosol samples from three major hospitals involved in COVID-19 care in Kuwait was collected. Viral RNA was isolated and subjected to comprehensive respiratory viral panel sequencing (CRVP) as per the standard protocol to detect the SARS-CoV-2 and other respiratory viruses in the hospital aerosol and monitor variations within the sequences. RT-PCR was also employed to estimate the viral load of SARS-CoV-2.
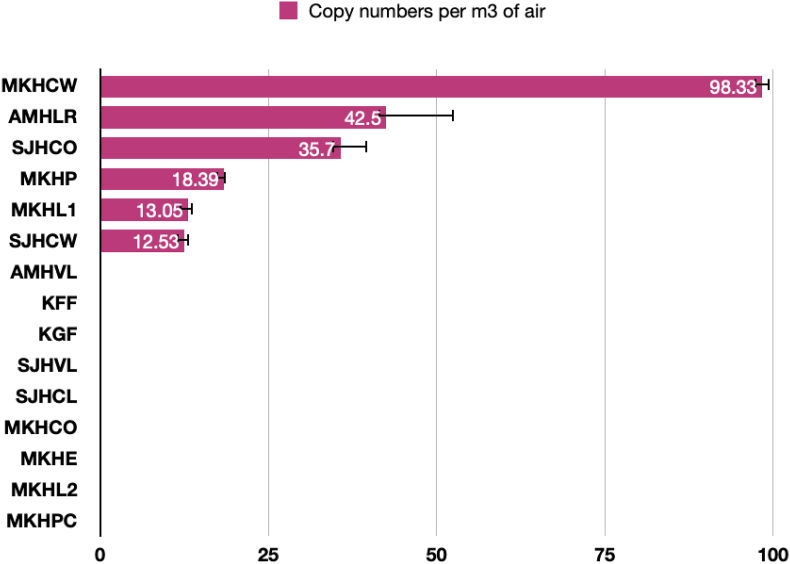
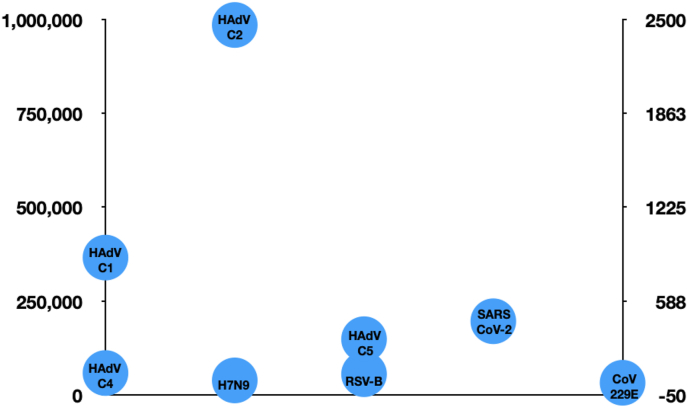
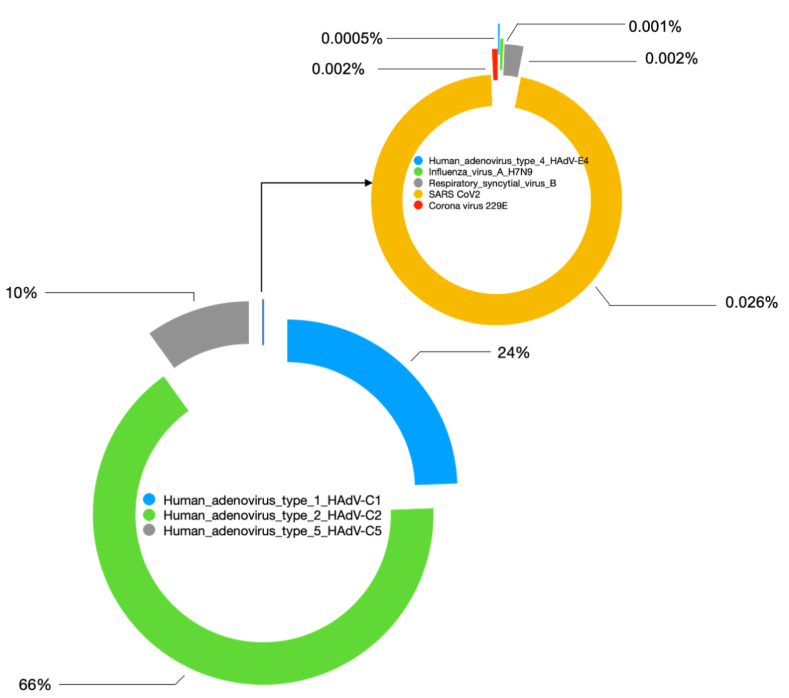
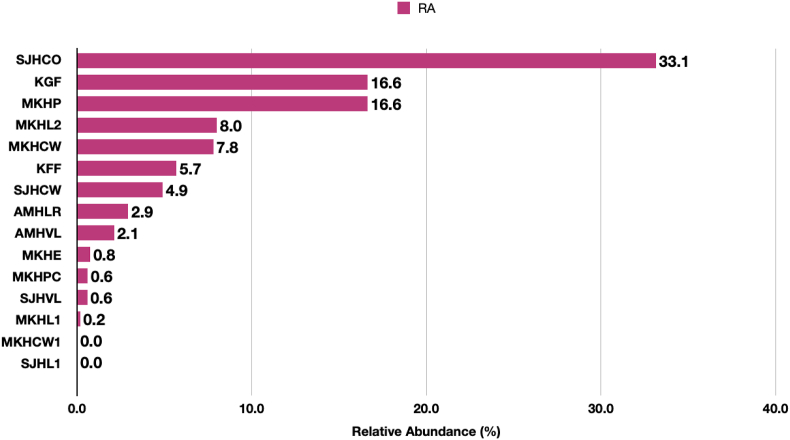
Findings: 13 of 15 (86.7%) samples exhibited SARS-CoV-2 with a relative abundance of 0.2-33.3%. The co-occurrence of human adenoviruses (type C1, C2, C5, C4), respiratory syncytial virus (RSV), influenza B, and non-SARS-CoV-229E were also recorded. Alignment of SARS-CoV-2 sequences against the reference strain of Wuhan China revealed variations in the form of single nucleotide polymorphisms (SNPs-17), insertions and deletions (indels-1). These variations were predicted to create missense (16), synonymous (15), frameshift (1) and stop-gained (1) mutations with a high (2), low (15), and moderate (16) impact.
Conclusions: Our results suggest that using CRVP on a large volume aerosol sample was a valuable tool for detecting SARS-CoV-2 in indoor aerosols of health care settings. Owing to its higher sensitivity, it can be employed as a surveillance strategy in the post COVID times to act as an early warning system to possibly control future outbreaks.
Keywords: Hospital infection; Mutations; Next-generation sequencing; RT-PCR; SARS-CoV-2; Surveillance.
© 2021 The Authors.
Figures
References
-
- Stockwell R.E., Ballard E.L., O'Rourke P., Knibbs L.D., Morawska L., Bell S.C. Indoor hospital air and the impact of ventilation on bioaerosols: a systematic review. Journal of Hospital Infection. 2019;103(2):175–184. - PubMed
-
- Habibi N., Uddin S., Al Salameen F., Al Amad S., Kumar V., Al Otaibi M. 2021. Identification and characterization of novel corona and associated respiratory viruses in aerosols.
LinkOut - more resources
Full Text Sources
Miscellaneous
