

Accuracy and Reliability of Single-Camera Measurements of Ankle Clonus and Quadriceps Hyperreflexia
- PMID: 34977536
- PMCID: PMC8683842
- DOI: 10.1016/j.arrct.2021.100153
Accuracy and Reliability of Single-Camera Measurements of Ankle Clonus and Quadriceps Hyperreflexia
Abstract
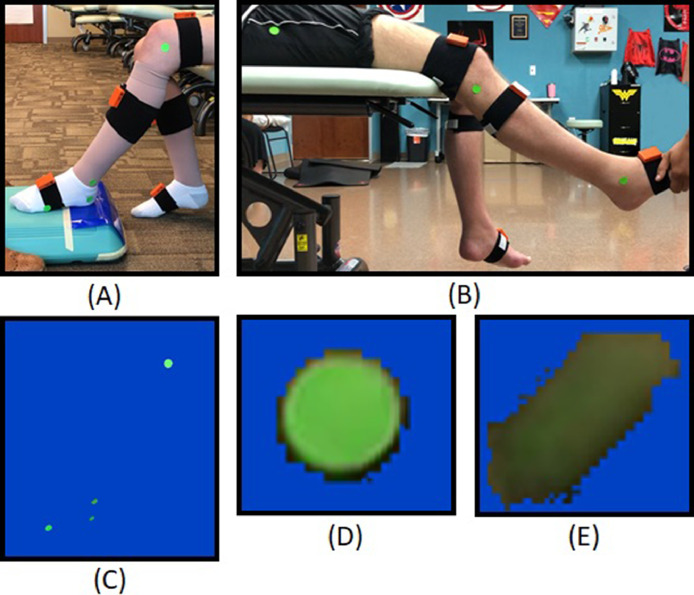
Objective: To evaluate the accuracy and reliability of a simple, single-camera smartphone-based method, named the Reflex Tracker (RT) system, for measuring reflex threshold angles related to ankle clonus and quadriceps hyperreflexia.
Design: A prospective comparison study using a high-fidelity reference standard was constructed employing a 2 × 2 × 2 factorial design, with factors of rater (tester) type (student and experienced physical therapist), joint (ankle and knee), and repetition (2 per condition).
Setting: This multicenter study was conducted at 4 outpatient rehabilitation clinics.
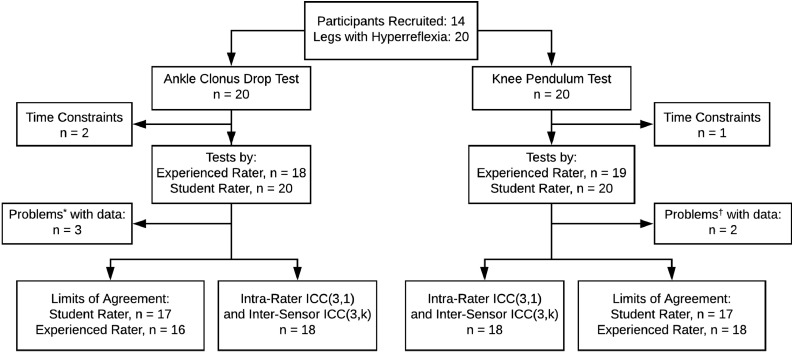
Participants: A convenience sample of 14 individuals with a neurologic condition presented with 20 lower limbs that exhibited ankle clonus and/or quadriceps hyperreflexia and were included in the study. Also participating in the study were 8 student and 8 experienced physical therapist raters (testers) (N=16).
Interventions: Not applicable.
Main outcome measures: The plantar flexor reflex threshold angle (PFRTA) related to ankle clonus and the quadriceps reflex threshold angle (QRTA) related to quadriceps hyperreflexia were quantified.
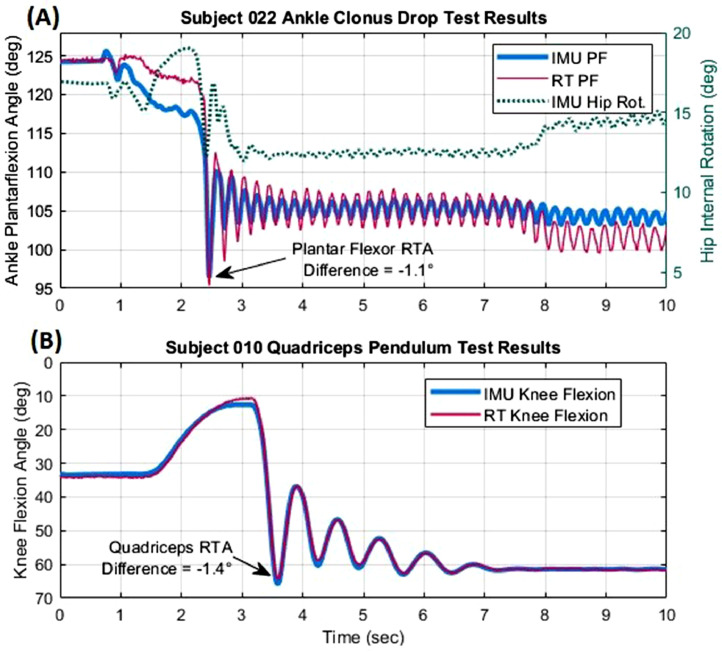
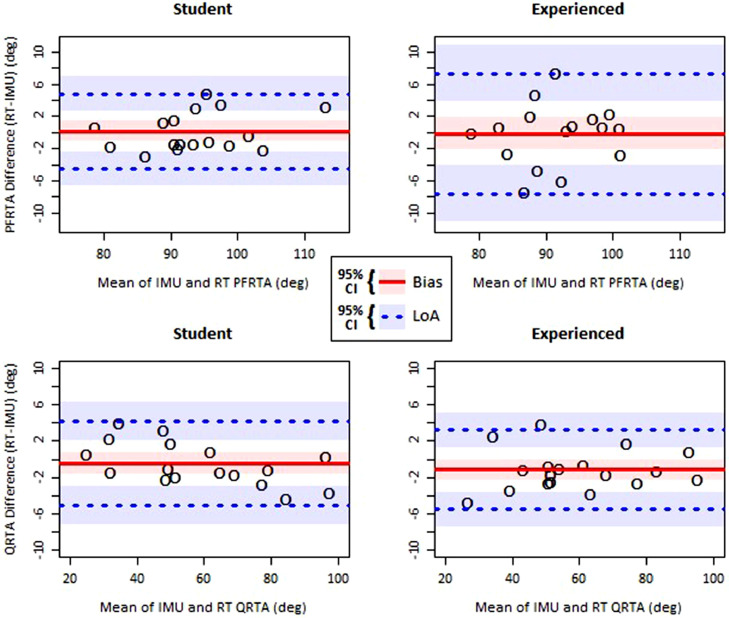
Results: PFRTA and QRTA results were compared between the smartphone RT method and synchronous 3-dimensional inertial measurement unit (IMU) sensor motion capture. Mean difference (bias) was minimal between RT and IMU measurements for PFRTA (bias≤0.2°) and QRTA (bias≤1.2°). Intrarater reliability for PFRTA ranged from 0.85-0.90 using RT and from 0.85-0.87 using IMU; QRTA ranged from 0.97-0.98 using RT and from 0.96-0.99 using IMU. Intersensor reliability for PFRTA and QRTA was 0.97 and 0.99, respectively. Minimum detectable change for PFRTA ranged from 7.1°- 8.7° and for QRTA ranged from 6.1°-8.3°.
Conclusions: RT performed comparable to IMU for accurate and reliable measurement of PFRTA and QRTA to quantify ankle clonus and quadriceps hyperreflexia in clinical settings.
Keywords: CI, confidence interval; ICC, intraclass correlation coefficient; IMU, inertial measurement unit; LSD, least significant difference; LoA, limit of agreement; MDC, minimum detectable change; PFRTA, plantar flexor reflex threshold angle; Plantar flexor; QRTA, quadriceps reflex threshold angle; RMS, root mean square; RT, Reflex Tracker; RTA, reflex threshold angle; Reflex threshold angle; Rehabilitation; Smartphone; Spasticity.
© 2021 The Authors.
Figures
Similar articles
-
Temporal Indices of Ankle Clonus and Relationship to Electrophysiologic and Clinical Measures in Persons With Spinal Cord Injury.J Neurol Phys Ther. 2017 Oct;41(4):229-238. doi: 10.1097/NPT.0000000000000197. J Neurol Phys Ther. 2017. PMID: 28922314
-
Reliability and validity of estimated angles information assessed using inertial measurement unit-based motion sensors.Biomed Mater Eng. 2024;35(5):439-450. doi: 10.3233/BME-240031. Biomed Mater Eng. 2024. PMID: 39031336
-
Tonic Stretch Reflex Threshold as a Measure of Ankle Plantar-Flexor Spasticity After Stroke.Phys Ther. 2016 May;96(5):687-95. doi: 10.2522/ptj.20140243. Epub 2015 Oct 8. Phys Ther. 2016. PMID: 26450971
-
Are tibial angles measured with inertial sensors useful surrogates for frontal plane projection angles measured using 2-dimensional video analysis during single leg squat tasks? A reliability and agreement study in elite football (soccer) players.J Electromyogr Kinesiol. 2019 Feb;44:21-30. doi: 10.1016/j.jelekin.2018.11.005. Epub 2018 Nov 10. J Electromyogr Kinesiol. 2019. PMID: 30469107
-
Contributions to the understanding of gait control.Dan Med J. 2014 Apr;61(4):B4823. Dan Med J. 2014. PMID: 24814597 Review.
Cited by
-
Collection of the digital data from the neurological examination.NPJ Digit Med. 2025 May 1;8(1):234. doi: 10.1038/s41746-025-01659-2. NPJ Digit Med. 2025. PMID: 40312534 Free PMC article.
References
-
- Gracies J. Pathophysiology of spastic paresis. II: emergence of muscle overactivity. Muscle Nerve. 2005;31:552–571. - PubMed
-
- Fee J, Miller F. The Leg Drop Pendulum Test performed under general anesthesia in spastic cerebral palsy. Dev Med Child Neurol. 2004;46:273–281. - PubMed
-
- Adams M, Hicks A. Spasticity after spinal cord injury. Spinal Cord. 2005;43:577–586. - PubMed
-
- Patrick E, Ada L. The Tardieu Scale differentiates contracture from spasticity whereas the Ashworth Scale is confounded by it. Clin Rehabil. 2016;20:173–182. - PubMed
LinkOut - more resources
Full Text Sources
