

Rescue transventricular off-pump mitral valve repair with artificial neochords for acute mitral regurgitation due to postinfarction papillary muscle rupture
- PMID: 34977729
- PMCID: PMC8691823
- DOI: 10.1016/j.xjtc.2021.09.047
Rescue transventricular off-pump mitral valve repair with artificial neochords for acute mitral regurgitation due to postinfarction papillary muscle rupture
Abstract
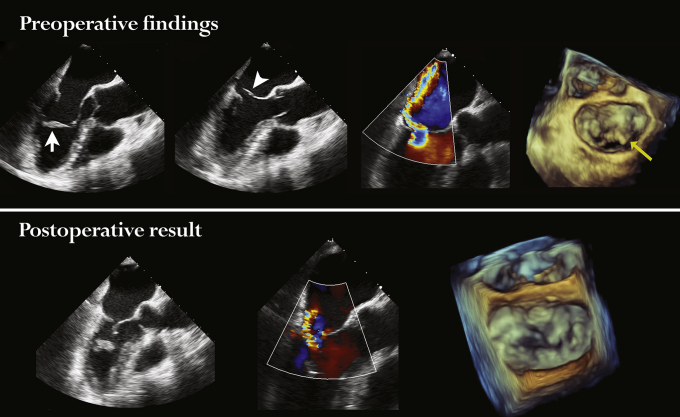
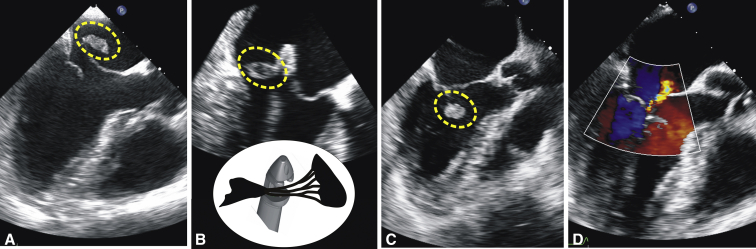
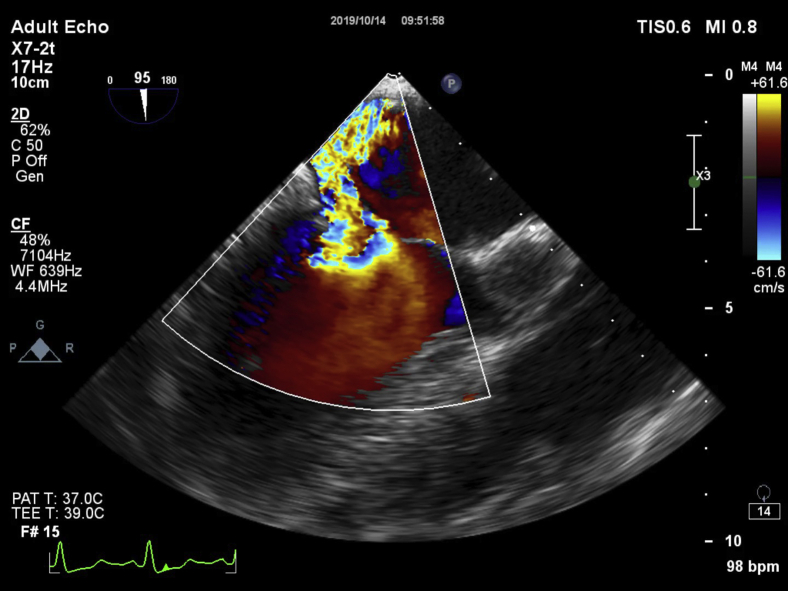
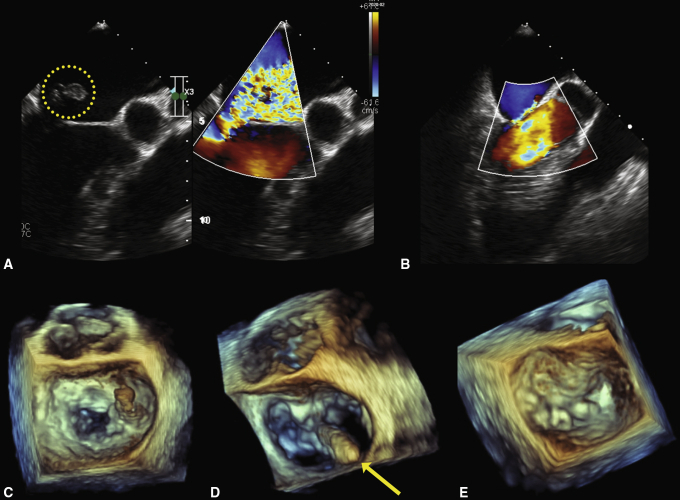
Background: We report 3 cases of rescue transventricular off-pump mitral valve (MV) repair in high-risk patients with acute mitral regurgitation (MR) due to post-myocardial infarction (MI) papillary muscle rupture (PMR).
Methods: The 3 patients presented with acute inferior ST elevation myocardial infarction, cardiogenic shock, and pulmonary edema. Their preoperative peak troponin I levels were 1909 ng/L, 16,963 ng/L, and 8299 ng/L. All 3 patients underwent successful percutaneous intervention to the culprit coronary artery, and antiplatelet therapy was initiated. All patients required inotropic support and had an intra-aortic balloon pump inserted preoperatively. Transesophageal echocardiography (TEE) demonstrated severe eccentric MR due to the leaflet prolapse secondary to PMR. The patients' estimated EuroSCORE II scores were 16.03%, 16.68%, and 7.81%, and their Society of Thoracic Surgeons scores were 14.77%, 18.24%, and 9.8%, respectively. All 3 patients underwent urgent transventricular off-pump MV repair using artificial chords, with 2 or 3 three neochords implanted. The duration of operation was <2 hours, and intraoperative and postoperative drainage was minimal in all cases. MV function was assessed by qualitative and semiquantitative TEE.
Results: Intraoperative MR reduction to a mild level was achieved in all 3 patients. All patients had moderate MR at discharge, likely due to left ventricular remodeling. Severe MR recurred in all patients, at 5, 4, and 2 months of follow-up, respectively. All 3 patients underwent an elective MV reoperation via conventional approach.
Conclusions: Off-pump transventricular MV repair may offer a safe and feasible alternative to stabilize high-risk patients with acute MR due to post-MI PMR. Although early MR recurrence is concerning, urgent transventricular MV repair may serve as a bridge to conventional surgery in such unstable patients.
Keywords: AF, atrial fibrillation; ECG, electrocardiography; IABP, intra-aortic balloon pump; LAD, left anterior descending artery; LV, left ventricular; LVEF, left ventricular ejection fraction; MI, myocardial infarction; MR, mitral regurgitation; MV, mitral valve; PCI, percutaneous coronary intervention; PMR, papillary muscle rupture; RCA, right coronary artery; STEMI, ST elevation myocardial infarction; STS, Society of Thoracic Surgeons; TEE, transesophageal echocardiography; TR, tricuspid regurgitation; acute mitral regurgitation; artificial chords; cardiogenic shock; minimally invasive; mitral valve; off-pump; papillary muscle rupture; transventricular mitral repair.
© 2021 The Author(s).
Figures



Comment in
-
Commentary: A shoestring catch….JTCVS Tech. 2021 Oct 27;10:243. doi: 10.1016/j.xjtc.2021.10.046. eCollection 2021 Dec. JTCVS Tech. 2021. PMID: 34984384 Free PMC article. No abstract available.
References
-
- Braunwald E. In: Heart Disease: A Textbook of Cardiovascular Medicine. 4th ed. Braunwald E., editor. WB Saunders; Philadelphia: 1992. Valvular heart disease.
-
- Sultan I., Aranda-Michel E., Gleason T.G., Navid F., Kilic A. Mitral valve surgery for acute papillary muscle rupture. J Card Surg. 2018;33:484–488. - PubMed
-
- Wei J.Y., Hutchins G.M., Bulkley B.H. Papillary muscle rupture in fatal acute myocardial infarction: a potentially treatable form of cardiogenic shock. Ann Intern Med. 1979;90:149–152. - PubMed
-
- Austen W.G., Sokol D.M., DeSanctis R.W., Sanders C.A. Surgical treatment of papillary-muscle rupture complicating myocardial infarction. N Engl J Med. 1968;278:1137–1141. - PubMed
-
- Figueras J., Calvo F., Cortadellas J., Soler-Soler J. Comparison of patients with and without papillary muscle rupture during acute myocardial infarction. Am J Cardiol. 1997;80:625–627. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
